
Strabismus: surgery
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The purpose of the operation with strabismus on the extraocular muscles is to achieve the correct position of the eyes and, if possible, restore binocular vision. However, the first stage in the treatment of pediatric strabismus is the correction of any significant abnormalities of refraction and / or amblyopia.
As soon as the maximum possible visual functions are achieved on two eyes, any residual deviation must be surgically eliminated. There are 3 basic operations with strabismus: weakening, reducing the traction force, strengthening, increasing the traction force, changing the direction of the muscle.
 [
[Strabismus: operations that weaken the action of muscle
There are 3 types of operations that weaken the action of the muscle: recession, myectomy, posterior fixation sutures.
Recession
This weakening of the muscle by moving the place of attachment to the back towards the beginning of the muscle. The recession can be carried out on any muscle, except the upper oblique.
Direct muscle recession
- after the exposure of the muscle, two absorbable sutures are placed on the outer quarter of the width of the tendon;
- the tendon is cut off from the sclera, the magnitude of the recession is measured and marked on the sclera with a compass;
- The stump is sewn to the sclera posterior to the original attachment site.
Recession of the lower oblique muscle
- Exposure of the abdomen of the muscle is achieved through the lower temporal arcuate incision;
- One or two absorbable sutures are applied to the muscle near the place of attachment;
- the muscle is cut off, and the stump is sutured to the sclera 2 mm from the temporal margin (attachment points of the lower rectus muscle).
Strabismus: operation of a myectomy
The procedure involves cutting the muscle at the site of attachment without further connection. This technique is most often used to reduce the hyperfunction of the lower oblique muscle. On the direct muscles this intervention is very rarely performed with a large muscle contraction.
Strabismus: the operation of the back fixing sutures
The principle of this intervention (Faden surgery) is to reduce the strength of the muscles in the direction of their action without changing the attachment site. The Faden operation can be used in DDA, and also to weaken horizontal straight muscles. When correcting the DVD, it is usually primarily the recession of the upper rectus muscle. The abdomen of the muscle is then sutured to the sclera with a non-absorbable filament 12 mm away from the place of attachment.
Strabismus: muscle strengthening operations
- Resection of the muscle enhances its effective traction. This procedure is suitable only for rectus muscles and includes the following interventions:
- a) after the exposure of the muscle, two absorbable sutures are passed through the muscle at the marked points to the rear of the attachment site;
- b) part of the muscle is excised anteriorly from the sutures, and the stump is sewn to the original attachment site;
- The formation of muscle or tendon folds is usually used to enhance the action of the upper oblique muscle with congenital paresis of the IV pair of cranial nerves.
- Moving (attaching the muscle closer to the limb) can provide an increase in action after a previous recession of the rectus muscle.
Treatment of paralytic strabismus
Paralysis of the external rectus muscle
Surgical intervention in case of paralysis of the VI pair of cranial nerves should be carried out only if there is no spontaneous improvement, which can be judged no earlier than 6 months later. There are 2 main interventions that improve abduction:
Operation Hummelsheim
- recession of the internal rectus muscle;
- the lateral halves of the upper and lower rectus muscles are cut off and hemmed to the upper and lower margins of the paretic lateral rectus muscles.
Since all three muscles are cut off from the eyeball with this intervention, there is a risk of postoperative ischemia of the anterior segment. In order to avoid this complication, the recession of the internal rectus muscle can be replaced by chemodenervation with CI toxin. Botulinum.
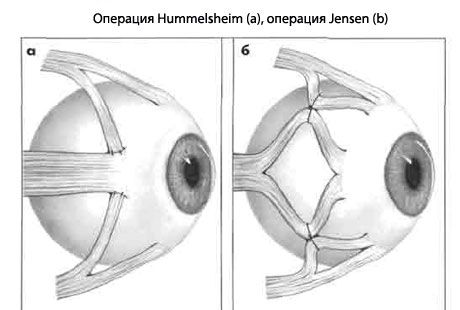
Operation Jensen improves abduction, and it is combined with recession or with injection of toxin CI. Botulinum into the external rectus muscle.
- the upper, outer and lower rectus muscles are split along the length;
- with the help of non-absorbable threads, the outer half of the upper rectus muscle is fixed to the upper half of the external straight line, and the lower half of the outer straight line to the outer half of the lower straight line.
Paralysis of the superior oblique muscle
Surgical intervention is indicated in the forced position of the head and diplopia, which is not eliminated by prisms.
- Congenital hypertrophy with a large angle in the primary position. In this case, the fold of the upper oblique muscle is performed.
- Acquired
- small hypertropy is corrected by ipsilateral diminution of the lower oblique muscle;
- acquired hypertropies with a medium and a large angle are eliminated by ipsilateral diminution of the lower oblique muscle, combined with ipsilateralal easing of the superior rectus and / or contralateral weakening of the superior rectus muscle. It should be taken into account that the weakening of the lower oblique and upper rectus muscles of the same eye can lead to hyper-elution;
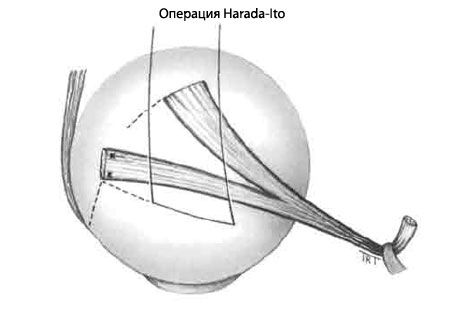
- Hypertrophic excretions are eliminated by the Harada-Ito operation, involving cleavage and anterolateral transposition of the outer half of the tendon with the upper oblique.
Strabismus: adjustable stitches
Indications
In some cases, the best results of surgical treatment are provided by the technique of controlled sutures. Special indications are the need for the correct position of the eyes and cases where the results of traditional interventions are difficult to predict. For example, the acquired vertical deviations with endocrine myopathy or the effects of a punctured fracture of the bottom of the orbit. Other relative indications are paralysis of the sixth pair of cranial nerves, exotrophy of adults, and repeated operations in scarring of surrounding tissues, when the result of the operation may be unpredictable. The main contraindication is the young age of the patient or the inability to post-operatively regulate the sutures.
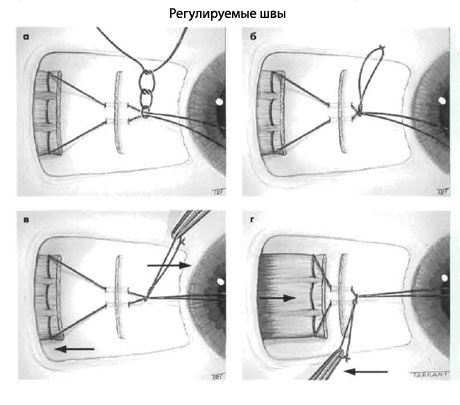
The first stages
- Exposure of the muscle, sutures are applied, the tendon is cut off from the sclera (as in the recession of the rectus muscle).
- The two ends of the thread are held close together through the stump at the attachment point.
- The second seam is tied and tightly tightened around the muscle seam in front to protect it from the stump.
- One of the ends of the seam is cut and the two ends are tied together, forming a loop.
- The conjunctiva remains open.
Postoperative regulation
- Assess the position of the eyes.
- If the position of the eyes is satisfactory, the muscular suture is tied and the long ends of the thread are shortened.
- If a large recession is required, the node is pulled anteriorly along the muscle seam, providing additional relaxation of the recessive muscle, and pushing it backward.
- If a smaller recession is required, the muscle suture extends anteriorly, and the knot is pulled and the direction opposite to the muscle stump.
- The conjunctiva is sutured.
A similar technique is used when resecting the rectus muscle.
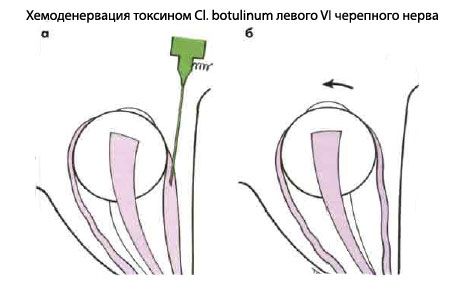
Strabismus: chemodenervation with CI toxin. Botulinum
Temporary paralysis of the extraocular muscle can be created in addition to the transposition described earlier, or in isolation. The main indications for chemodenervation:
- To determine the function of the external rectus muscle in case of paralysis of the VI pair of cranial nerves, in which the contracture of the internal rectus muscle interferes with abduction. A small dose of toxin CI. Botulinum is injected into the abdomen of the antagonist in hyperfunction (internal rectus muscle) under electromyographic control. The temporary paralysis of the muscle causes it to relax, and the action of the horizontal muscles of the eye is balanced, allowing you to evaluate the function of the external rectus muscle.
- To determine the risk of postoperative diplopia and assess the potential of binocular vision. For example, in an adult patient with a diverging strabismus on the left and a high visual acuity in both eyes, injection of a toxin CI. Botulinum in the external rectus muscle of the left eye will lead either to straightening the position of the eyes, or to convergence.
However, placing a corrective prism in front of the deflected eye is often a more simple and accurate method for assessing the risk of postoperative diplopia. If one of the ways indicates the possibility of diplopia, the patient can be informed about this. However, such diplopia, as a rule, spontaneously disappears.