
Visual acuity: visual acuity check
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Central vision is the vision that determines the perception of an object, fixed by a glance. Central vision is carried out by the sensors of the central fossa of the yellow macula of the retina and is characterized by the greatest visual acuity. The impulse from each cone of the central fossa of the retina passes through individual nerves through all parts of the optic path, which guarantees a higher visual acuity.
Spatial visual acuity is the ability to distinguish individual elements of an object or perceive it entirely. Quantitatively equivalent to the minimum angle of discrimination, calculated from the nodal point of the eye between two objects, allowing them to be seen separately. The minimum angle of discrimination is 1 arc minute or less, which corresponds to line 6/6 on Snellen optotypes from a distance of 6 m.
Visual acuity is the sensitivity of the visual analyzer, which reflects the ability to distinguish the components and boundaries of visible objects; oriented by the minimum angular distance between the two points, at which they are perceived separately. The smallest angular distance corresponds approximately to one minute, at this value the magnitude of the image on the retina is 0.004 mm, which corresponds to the diameter of the cone. The visual analyzer is capable of catching objects that are larger than the diameter of the cone. The component parts of the object are different, when the excited cones are separated even by one unexcited one.
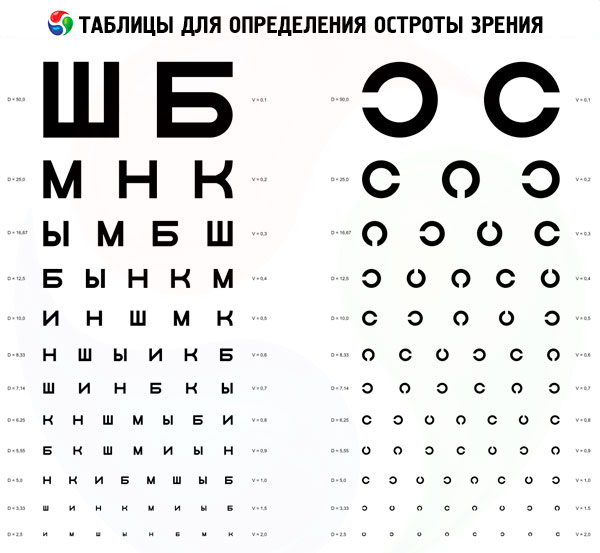
To study visual acuity, special tables are used, containing different magnitudes of optotypes (letters, numbers, signs).
Indications for checking visual acuity
Complaints of the patient for vision loss. Visual acuity is also determined during preventive examinations.
Preparation for the determination of visual acuity
Equipment: Rota apparatus, Golovin-Sivtsev table (children's visometric tables), pointer, bright light source (for determining the light projection).
Before the procedure for determining visual acuity, the patient explains the procedure for the study.
Methodology and interpretation of visual acuity testing
The patient sits at a distance of 5 meters from the table. The study of visual acuity is carried out alternately: first for the right (OD), then for the left (OS) eye. The eye that does not take part in the study is covered with a scutellum (a sheet of paper, palm). The symbols of the table are presented within 2-3 seconds and ask the examinee to name them. Observe that the pointer does not interfere with reading the symbols. The visual acuity is determined by the symbols of the minimum size that the patient recognizes. When reading the first 7 lines of errors can not be; beginning with the 8th line, one error in the line is neglected (visual acuity is indicated in any row to the right of the optotypes).
Example of data registration: Visus OD = 1.0; Visus OS 0.6.
If the visual acuity is less than 0.1 (the patient does not see from the distance of 5 meters of the 1st line of the table), bring it to the distance (d) from which it will be possible to name the symbols of the 1st row (the usual eye recognizes the symbols of this row with 50 m, D = 50 m). Calculation using the Snellen formula:
Visus = d / D (m),
Where Visus (Vis, V) - visual acuity;
D is the distance from which the patient reads the 1st row:
D is the calculated distance from which the component parts of the symbols of this series are visible at a viewing angle of 1 (indicated in any row to the left of the optotypes).
In case the patient does not recognize the symbols of the 1st row from a distance of 50 centimeters, the visual acuity is characterized by the distance from which he has the opportunity to count the doctor's extended fingers (example: Visus OD = finger count from a distance of 15 centimeters from person). In case the patient does not have the opportunity to count fingers, although he sees the movement of the hand in the face, the visual acuity data is written as: Visus OS = moving the hand of the person.
The lowest visual acuity is the ability of the eye to distinguish light from darkness; this is checked in a darkened room when the eyes are illuminated by a clear light beam. In case the patient sees light, the visual acuity is equal to the light perception (Visus OD = 1 / *, or perceptio lutis). By directing a beam of light around the eyes (from above, from below, from the right, from the left), we check how the ability of individual parts of the retina to retain light. The correct answers show the correct projection of light (Visus OD = 1 / * proectio lucis certa). When the opaque media of the eye (cornea, lens, CT) become clouded, visual acuity can be reduced to light, but the projection of light is almost always determined correctly. With an erroneous projection of light, it is necessary to show from which side the patient sees light (for example, light sensation from the side of the temple, from above and from below).
The absence of the right projection of light (perceptio et proectio lucis incerta) or absolute absence of light perception (Visus = O) in the subject indicates a lesion of the retina or optic nerve.
In the English-speaking states, visual acuity is traditionally determined from a distance of 20 feet or 6 meters (one foot 30.5 cm) and is written according to Snellen's formula in the form of a fraction.
Verification of visual acuity in children in the preverbal phase of development
Comparative evaluation of the eyesight of both eyes is carried out by simple observation of the child.
- Covering one eye, negatively perceived by the child, indicates a low visual acuity of the pair eye.
- The fixation test is carried out as follows:
- a prism in a 16D base is placed down in front of one eye, the other eye is covered;
- The eye behind the prism is deflected upward, holding the fixation;
- observe the eye behind the prism;
- fixation is assessed as central or non-central, stable or unstable;
- open another eye and determine the ability to restrain fixation;
- if the slightly opened eye becomes fixative, the visual acuity is reduced;
- if after blinking the fixation remains, visual acuity is high;
- if the fixation alternates, the visual acuity in both eyes is the same;
- the test is repeated by placing a prism in front of the other eye;
- Monocular fixation should be central, stable and supported by each eye.
- The test "Hundreds and thousands of sweets" is a great test, which is rarely carried out. Usually a child is able to see and pick up small sweets at a distance of 33 cm with a visual acuity of at least 6/24.
- Rotational test - quantitative, assesses the child's ability to fix his eyes with two open eyes. Carried out as follows:
- The examiner keeps the child facing him and quickly rotates it around 360;
- with normal vision, the child's eyes are directed towards the rotation under the influence of the vestibular-ocular reflex. The eyeballs return intermittently to the primary position, which is accompanied by a rotational nystagmus;
- when the rotation stops, the nystagmus disappears when suppressing the constructive nystagmus by fixation;
- if the vision is significantly reduced, the induced nystagmus does not disappear after cessation of rotation, since the vestibular-ocular reflex is not blocked by the principle of reverse visual communication.
- Methods of preferential fixation of the eye can be applied from infancy. Infants, as a rule, react to the pattern, and not to a homogeneous stimulus. The infant is shown a stimulus, and the examiner observes the fixation movements of the eyes. Examples of the stimulus can serve as Teller cards for the study of visual acuity, which consist of black bands of different thicknesses, and Cardiff cards, consisting of shapes with different contours. Thick stripes or shapes with thick contours (with a low spatial frequency) are seen better than with thin ones, according to this, and assess the visual acuity. With amblyopia, visual acuity determined by gratings is often higher than estimated with Snellen optotypes; in turn, visual acuity, determined by Teller cards, can also be overstated.
- The visual cortical potentials caused by pattern-stimulation reflect a spatial contrast sensitivity. They are used, mainly, for the diagnosis of optical and neuropathy.
- Optokinetic nystagmus may indicate visual acuity, depending on the size of the bands.
Verification of visual acuity in children in the verbal phase of development
- At the age of 2 years, most children acquire sufficient language skills for naming optotypes, for example, according to the Cow.
- At the age of 3, most children can recognize individual optotypes of the Sheridan-Gardiner test. The disadvantage of this method is an overestimation of visual acuity with amblyopia, since it does not cause the phenomenon of "crowding". The Keeler LogMAR test is close to the tables and is more accurate for determining visual acuity in amblyopia, as it requires the selection of a pair from the group of optotypes from the child.
- By the age of 4, in most children, visual acuity can be checked on the Snellen tables.
Study of stereopsis
Stereopsis is measured in arc seconds (1 = 60 arc minutes, 1 arc minute = 60 arc seconds). It must be remembered that the normal spatial visual acuity is 1 arc minute, and the normal stereo stitch is 60 seconds (which corresponds to 1 minute). The lower the value, the higher the sharpness.
Test Titmus
This is a three-dimensional polaroid vector in the form of a booklet, consisting of two tables, considered by the patient through polaroid glasses. On the right side of the booklet is a large fly, on the left - circles and animals. The test is carried out at a distance of 405 mm.
- "Fly" is a test for rough stereopsis (3000 arc seconds), especially informative for young children. The fly should look bulky, and the child is offered to "lift" it for one of the wings. In the absence of a coarse stereopsis, the fly looks flat, as in the photo (if you turn the booklet over, the image becomes flat). If the patient insists that the fly's wings protrude, the evaluation of stereoscopic vision is incorrect.
- "Circles" - a series of step-by-step tests for evaluating stereoscopic vision. Each of the squares consists of 4 circles. Each of the circles has a certain degree of dysiaricity and, under normal stereopsis, protrudes in front of the plane. The severity of stereoscopic vision is calculated from the table attached to the test. The angle of disparatiosity is from 800 to 40 arc seconds. If the patient sees a shift of the circle to the side, he does not have stereoscopic vision, but is oriented monocularly.
- «Animals». The test is similar to a test with circles and consists of 3 rows of animals, one of which protrudes in front of the plane. The degree of desiarality is from 400 to 100 arc seconds.
Test TNO
The test "Random points" consists of 7 tables, viewed through red-green glasses. Each table contains various figures (squares, crosses, etc.) formed from random points of complementary colors. Some figures are visible without red-green glasses, while others are "hidden" and visible only if there is a stereoscopic view in the red-green glasses. The first three tables are designed to identify stereoscopic vision, and the following are for quantitative evaluation. Since monocular "hints" do not contain the TNO test, it more accurately measures the stereopsis than the Tiimus test. Disparity is from 480 to 15 arc seconds.
Test Lang
For this test, no special glasses are required. Objects are visualized separately with each eye through the built-in elements with cylindrical lenses. Displacement of points creates disparity. The patient is asked to name or show a simple figure on the card, for example, a star. The Lang test is especially informative for assessing stereopsis in young children and infants, as they instinctively stretch their hands and point to pictures. The examiner can observe the movements of the child's eyes from one picture to another. Dysparativity ranges from 1200 to 600 arc seconds.
The Frisby test
The test consists of 3 transparent plastic plates of different thicknesses. On the surface of each plate are printed 4 squares with small random figures. In one of the squares there is a "Hidden" circle, within which figures are printed from the back of the plate. From the patient it is required to reveal this hidden circle. The test does not require special glasses, since dysparathy is created by the thickness of the plate and can be varied by approaching and removing the plate. Dysparativity is from 600 to 15 arc seconds.
Prism base to the outside
Fast in execution and an easy way to identify binocular vision in children who can not be held stereotests. The test is carried out as follows: a prism of 20 D is placed with a base outside before the eye (in this case, the right one). This shifts the retinal image to the temple, inducing diplopia. The examiner observes the installation movement:
- right eye movement to the left to restore fixation (adduction to the right) with the corresponding movement of the left eye to the left (abduction from the left) in accordance with the law Hering;
- the left eye makes the setting movement to the right (reductduction from the left);
- removing the prism, observe the movement of both eyes to the right;
- The left eye produces a movement to the right to restore fusions.
Most children with good binocular vision must overcome the prism by force in 20 D. Otherwise, we need to use weaker prisms (16 D or 12 D).
Investigation of sensory anomalies
Four-Point Test Worth
Conducting
- the patient is put a red lens in front of the right eye, which cuts off all colors except red; before the left eye put a green lens that cuts off all the colors except the green;
- the patient is shown a drum with 4 circles: 1 - red, 2 - green and 1 - white.
results
- All the figures are visible - normal fusions.
- Visibility of all figures in the presence of a manifest form of strabismus testifies to ACS.
- The patient sees 2 red figures - suppression of the left eye.
- The patient sees 3 green figures - suppression of the right eye.
- The patient sees 2 red and 3 green figures - the presence of diplopia.
- If the green and red figures alternate, then there is an alternating suppression.
Striped glasses Bagolini
Each lens has the finest strips, and the point light source viewed through them becomes a line, similar to the Maddox stick.
Conducting
- two lenses with an angle of 45 and 135 are placed in front of each eye, and the patient fixes a point source of light;
- Each eye perceives an oblique line of light perpendicular to the line perceived by the pair eye;
- different images appear in front of each eye under biocular conditions.
The results can not be interpreted correctly, until the fact of the existence of the manifest strabismus is known.
- Two bands intersect in the center, forming an oblique cross ("X") - the patient has orthotropy or ACS.
- Two lines are visible, but not in the form of a cross - the patient has a diplopia.
- If only one band is visible, then simultaneous perception does not occur.
- In one of the bands there is a small gap - there is a central suppression scotoma.
Consecutive image
The test demonstrates the visual direction of the fovea.
Conducting
- One fovea is stimulated by a vertical strip of bright light, and the other by a horizontal strip;
- The vertical strip is more difficult to suppress, so it is projected onto the fovea of the mowing eye.
Results. The patient draws the relative position of consecutive images.
- Two consecutive images intersect in the form of a cross - the correspondence of the retina is normal.
- If two consecutive images do not intersect, then AKS is diagnosed.
- If the horizontal sequential image is projected onto the right fovea with esotropy with AKS, then it is visible to the left of the vertical image.
- The reverse results are obtained with exotropy.
- A patient with an eccentric fixation will also see a cross. Eccentric fixation is a one-sided state in which an extrafoveal part of the fovea is used for fixation in binocular and monocular conditions. Reorientation of sensory and motor functions occurs in such a way that this region usurps the main visual image belonging to the fovea. On the fovea of the dominant eye, the consecutive image is projected directly from the visual space. The consecutive image of the eccentric region of the mowing eye will also be projected directly from the visual space, as the region "lost" the main visual direction.
 [
[