Medical expert of the article

New publications
Williams syndrome
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Williams syndrome (Williams-Beuren, WS) is a genetic disorder characterized by distinctive facial features, mild to moderate cognitive impairment, learning disabilities, cardiovascular abnormalities (focal or diffuse stenosis of medium- to large-caliber arteries), and idiopathic hypercalcemia.
Often children with this diagnosis have amazing oratory skills, great success in musical art, and are distinguished by a high level of empathy.
Causes Williams syndrome
The causes of Williams syndrome are not yet fully understood, but it is known for sure that with this disease the paired set of chromosomes is preserved in a complete form.
The disorder manifests itself at the genetic level – part of the chromosome from the 7th pair is lost, which is why this missing section is not transmitted at the moment of conception. As a result, the child develops symptoms characteristic of Williams syndrome – each gene has its own “specialization”, therefore, in the absence of any of them, specific external and internal changes occur.
Since the pathology usually occurs spontaneously (due to a chromosomal mutation at conception), it can be concluded that the nature of the disease is congenital, not hereditary. Only in rare cases is the disease hereditary - when at least one of the parents has Williams syndrome.
Such genetic anomalies usually arise as a result of negative impact on the body of the child's parents - a "harmful" profession, poor ecology in the place of residence of the future father and mother, etc. But such gene mutations can also appear spontaneously, without any apparent reason.
 [ 4 ]
[ 4 ]
Pathogenesis
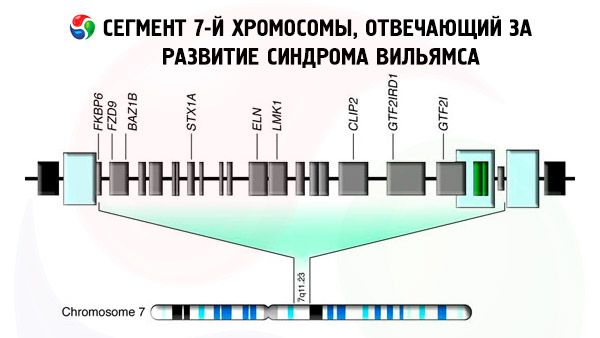
Almost all cases of Williams syndrome involve haploinsufficiency (i.e. loss of 1 of 2 copies) due to a deletion in chromosome 7, in the range 7q11.23, with the absence of the ELN gene responsible for elastin synthesis. The size of the deletion can vary.
Williams syndrome is caused not only by haploinsufficiency of elastin, but also by the deletion of a region that spans more than 28 genes and is therefore considered a contiguous gene deletion syndrome. Haploinsufficiency of elastin leads to the development of cardiovascular pathologies (including supravalvular aortic stenosis), connective tissue pathology and facial dysmorphology.
Other genes in the deletion region, such as LIMK1, GTF1IRD1, GTF2IRD2, GTF2I, NCF1, STX1A, BAZ1B, clip2, TFII-1, LIMK1 and a number of others affect the cognitive profile, the development of hypercalcemia, carbohydrate metabolism disorders and hypertension.
Symptoms Williams syndrome
Children with this syndrome have special facial features that resemble an elf. The disease was first described in 1961 by New Zealand pediatric cardiologist J. Williams, who studied the cardiovascular system of patients with mental retardation and characteristic manifestations in appearance.
Unlike other genetic disorders, children with Williams syndrome are generally social, friendly, and sweet. Parents often report that they do not notice any abnormalities in their children's mental development.
But there is another side to the coin. Many children have life-threatening cardiovascular diseases. Children with WS often require expensive and ongoing medical care and early psychological correction (such as speech training or occupational therapy), which may not be covered by insurance or government funding.
Many adults with this diagnosis work as volunteers or employees.
During school years, children often experience severe isolation, which can lead to depression. They are extremely sociable and have a normal need to interact with others, but often fail to understand the nuances of social interaction.
An unusual-looking face, mental retardation, and serious physical disabilities are the main signs of Williams syndrome. These include heart defects, flat feet or clubfoot, highly elastic joints, and problems with the musculoskeletal system. Malocclusion is often formed (since the teeth of such children erupt quite late). In addition, the teeth are small, widely spaced, irregularly shaped, and often affected by caries.
During the first 2 years of life, sick children are very weak - they eat poorly, they have a strong constant thirst, they often suffer from constipation, which is replaced by diarrhea, as well as vomiting. As they grow older, children acquire new distinctive features in appearance - an elongated neck, a narrow chest, a low waist.
If in infancy these children are significantly behind their peers in height and weight, then, as they grow older, they, on the contrary, begin to suffer from excess weight. Often, Williams syndrome is associated with metabolic problems - increased levels of calcium and cholesterol in the blood.
Diseases of the heart and blood vessels
Most people with Williams syndrome have heart disease (valvular aortic stenosis) and blood vessel disease (pulmonary artery stenosis, descending aorta, and intracranial arteries) of varying severity. Renal artery stenosis leads to hypertension in 50% of cases.
Hypercalcemia (high blood calcium)
Some children with WS have elevated blood calcium levels. The frequency and cause of this abnormality are unknown. Hypercalcemia is a common cause of irritability and "colic" in childhood.
In most cases, hypercalcemia resolves on its own in childhood without any treatment, but sometimes it persists throughout life.
Low birth weight/slow weight gain
Most children with Williams syndrome have a lower birth weight than their healthy peers. Slow weight gain is also common, especially during the first few years of life.
Feeding problems
Many young children have problems with breastfeeding. These include low muscle tone, a strong gag reflex, poor sucking/swallowing, etc.
Gastrointestinal diseases
Reflux gastritis, chronic constipation and diverticulitis of the sigmoid colon are frequently detected.
Endocrine pathology
Adults with Williams syndrome are more likely to be obese, have impaired glucose tolerance, and have diabetes mellitus than healthy individuals. They are also more likely to have an underdeveloped thyroid gland with subclinical hypothyroidism.
[ 16 ]
Kidney anomalies
Sometimes there are anomalies of the kidney structure with a violation of their functional capacity. Renal stone disease and bladder diverticula often develop.
Hernias
Inguinal and umbilical hernias are more common in Williams syndrome than in the general population.
Hyperacusis (sensitive hearing)
Children with this diagnosis have more sensitive hearing than other healthy children.
Musculoskeletal system
Young children often have low muscle tone and joint instability. As they get older, joint stiffness (contractures) may develop.
Excessive friendliness (sociality)
People with Williams syndrome are very nice. They have excellent public speaking skills and are very polite. They tend to be afraid of strangers and prefer to communicate with adults.
Mental retardation, learning disabilities and attention deficit disorder
Most people with WS have learning disabilities and cognitive impairments.
More than 50% of children with Williams syndrome have attention deficit disorder (ADD or ADHD), and about 50% have phobias, such as fear of loud noises.
By age 30, most people with WS have diabetes or prediabetes, mild to moderate sensorineural hearing loss (a form of deafness due to a problem with the auditory nerve).
First signs
When recognizing symptoms of Williams syndrome in a child, parents need to pay attention to how the child is developing in addition to external manifestations from an early age. Sick children have a weakened body and also lag behind their peers in development, both mentally and physically.
The physical development of sick children is normalized by the age of 3, but deviations in speech begin. But parents are not always able to identify the problem, since the baby is very sociable and active. Also among the signs indicating Williams syndrome is the timbre of the voice, hoarse and low.
Children with this disorder begin to speak quite late – it turned out that they say their first words only at 2-3 years old, and they can pronounce entire phrases only by 4-5 years old. The syndrome also causes problems with visual coordination and motor skills.
The movements of such children are jerky and rather awkward, they find it difficult to master even the most basic skills, they are unable to take care of themselves independently. But at the same time, they are very interested in music and show good musical abilities.
[ 21 ]
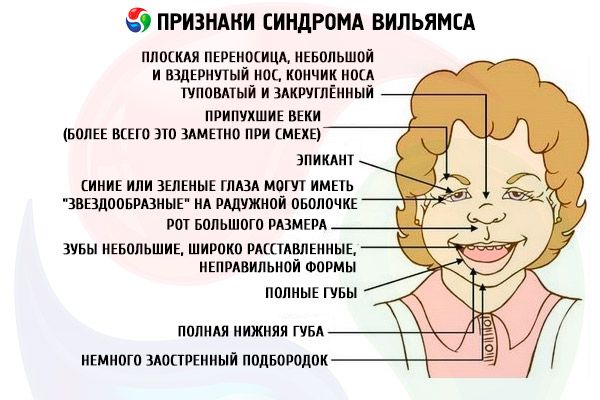
Elf face in Williams syndrome
People with Williams syndrome have distinctive facial features that resemble the face of an elf:
- Low position of the eyes, swollen eyelids (this is most noticeable when laughing);
- Large mouth with full lips and malformed bite;
- Disproportionately wide forehead;
- Full cheeks;
- The back of the head is convex;
- The bridge of the nose is flat, the nose itself is small and upturned, the tip of the nose is blunt and rounded;
- Slightly pointed chin;
- The ears are set quite low;
- Eyes are blue or green and may have noticeable "star-shaped" or white lace patterns on their irises. Facial features become more obvious with age.
Williams-Campbell syndrome
The so-called Williams-Campbell syndrome is a pathology that occurs due to congenital defective development of elastic and cartilaginous tissues in the distal part of the bronchi (2-3/6-8 branching sections). The defective structure of the bronchial wall causes their hypotonic dyskinesia - they expand sharply when inhaling and collapse when exhaling. Williams and Campbell in 1960 described the manifestation of generalized bronchiectasis in 5 children (the disorder arose due to congenital defective development of the bronchial framework).
The syndrome can be diagnosed at an early age - the disease manifests itself as chronic obstructive bronchitis. Among the main symptoms are stridor breathing, regular wet cough, shortness of breath with little physical exertion, weak voice.
Complications and consequences
Diagnostics Williams syndrome
The diagnosis of Williams syndrome is primarily determined based on chromosome analysis data. However, since some abnormalities cannot be determined by simple analysis, special genetic tests are also performed during the diagnostic process, which can confirm that a certain part of one chromosome of the 7th pair is missing.
Prenatal screening can reveal signs of polycystic dysplastic kidney disease, congenital heart defects, increased nuchal translucency in the fetus, and low levels of alpha-fetoprotein (MSAFP) in the mother's blood.
Tests
When diagnosing Williams syndrome, the following tests are performed:
- FISH test of chromosome parts to confirm the diagnosis;
- Blood sampling to determine creatinine levels;
- Urine test;
- Analysis of calcium levels in the blood serum, as well as determination of the ratio of creatinine and calcium levels in the urine.
Instrumental diagnostics
The following instrumental procedures are performed for Williams syndrome:
- Cardiodiagnostics is a complete clinical examination by a cardiologist who specializes in childhood diseases. The procedures include measuring blood pressure in the arms and legs, as well as an electrocardiogram.
- Diagnostics of the genitourinary system – ultrasound of the kidneys and ureter, as well as a study of the functional activity of the kidneys.
Differential diagnosis
In Williams syndrome, phenotypic manifestations of Noonan syndrome may be observed.
Treatment Williams syndrome
Since Williams syndrome is a genetic disorder, modern medicine is not yet able to cure it. There are only general supportive recommendations:
- Eliminate the child's need for additional vitamin D and calcium intake;
- If there is an elevated calcium level, it is necessary to try to reduce it;
- In case of narrowing of blood vessels (severe form), surgical treatment may be prescribed;
- Physiotherapy exercises to improve joint mobility;
- Advanced course in psychological and pedagogical development;
- Symptomatic therapy.
People with this diagnosis require regular monitoring of the cardiovascular system to avoid the development of arterial hypertension and heart failure.
Prevention
Preventive treatment methods for children with Williams syndrome.
Under 1 year of age:
- Closely monitor the risk of developing otitis media;
- When feeding, cope with the difficulties of the transition to solid food;
- Avoid taking multivitamin medications that contain vitamin D.
Ages 1-5 years:
- Monitor your diet;
- If necessary, undergo therapy courses: speech therapist, exercise therapy, sensory integration;
- Prevent the possibility of constipation;
- If a child has an unexplained increase in temperature, he or she should be checked for a urinary tract infection.
Ages 5-12:
- A proper diet along with regular physical activity (children with Williams syndrome often become overweight in early adolescence);
- Therapy aimed at reducing the child’s anxiety (relaxation techniques, consultations with a psychologist, medication treatment).
Ages 12-18:
- Discuss the illness with the teenager and refer him to a special support group;
- To assist in gaining independence;
- Encourage regular exercise, constant activity and movement;
- Encourage regular visits to doctors for gastrointestinal and urinary tract examinations;
- Monitor the teenager's mental health, tracking possible deviations.
Forecast
Although children with Williams syndrome increasingly lag behind their peers in intellectual development with age, thanks to their ability to listen, as well as their compliance and sociability, the prognosis for improving their mental state is favorable. In the process of teaching such children, it is necessary to take into account their spontaneity and excessive laughter, as well as their silly mood - therefore, classes should be held in a calm environment. It is also necessary to remove from the room all unnecessary objects that can distract the baby. Children with Williams syndrome should communicate with healthy peers - this has a beneficial effect on their further development.
Life expectancy
People with Williams syndrome have a shorter life expectancy than others.
Cardiovascular disease (coronary insufficiency) is the leading cause of early death in Williams syndrome.
Most experts associate it with elevated calcium levels, which causes calcification of the arteries and heart muscles at an early age. 75% develop supravalvular stenosis of the aorta, which sometimes requires surgery. Since people with this syndrome are highly susceptible to developing cardiovascular diseases, they are recommended to undergo preventive examinations every year.
[ 43 ]
Disability
Although Williams syndrome is a congenital genetic disorder, it is not a geneticist who refers such children for disability registration, but a psychiatrist. This is due to the fact that a child with genetic deviations has mental retardation, which can only be diagnosed by psychiatrists. It is the delay in mental development that prevents such a person from functioning normally, which is the basis for assigning him a disability.