Medical expert of the article

New publications
Uterine prolapse: causes, stages, diagnosis, and modern treatment methods
Last updated: 08.04.2026

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
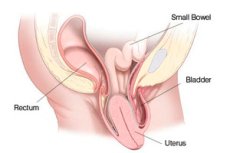
Uterine prolapse, or uterine prolapse, is a condition in which the uterus drops below its normal position due to weakening of the pelvic floor muscles and supporting ligaments. In modern gynecology, it is usually considered part of a broader group of conditions collectively known as pelvic organ prolapse. This means that a woman often experiences simultaneous displacement of not only the uterus, but also the anterior or posterior vaginal wall, the bladder, and sometimes the apex of the vagina after a previous hysterectomy. [1]
Uterine prolapse itself is not a life-threatening condition, but it can significantly impair quality of life. Symptoms typically include a feeling of heaviness, a "bulge," or bulge in the vagina, discomfort when walking, problems with urination, constipation, difficulty with intercourse, and a constant feeling of pressure in the lower abdomen. In some women, symptoms worsen in the evening, after prolonged standing, lifting, or straining. [2]
It's clinically important to understand that uterine prolapse doesn't always require immediate surgery. In some women, prolapse is mild, causes minimal discomfort, and can be observed. In others, symptoms become so noticeable that, without treatment, it becomes difficult to walk normally, work, exercise, have sex, or urinate or defecate normally. It is the severity of the symptoms, not just the anatomical stage, that determines the need for active treatment. [3]
A modern approach to uterine prolapse is based on a step-by-step approach. First, they determine what exactly is prolapsed, how severe it is, and what functions are impaired. Then, they discuss all realistic options: observation, lifestyle changes, pelvic floor muscle training, a vaginal pessary, organ-preserving surgery, or hysterectomy. A good modern approach begins not with the phrase "we need to operate," but with the phrase "we need to understand what exactly is interfering with this woman's life." [4]
Table 1. What is important to understand right away
| Question | Short answer |
|---|---|
| What is uterine prolapse? | Downward displacement of the uterus due to weakness of the supporting structures |
| It's always an isolated problem. | No, it is often associated with vaginal wall prolapse. |
| Is it life-threatening? | Usually no, but quality of life can suffer greatly |
| Is surgery always necessary? | No, observation and conservative treatment are possible. |
| What does tactics depend on? | Depending on symptoms, stage, age, associated diseases and pregnancy plans |
Sources for the table: [5]
Code according to ICD 10 and ICD 11
In the International Classification of Diseases, 10th revision, uterine prolapse is classified under the headings of prolapse of the female genital organs. The most commonly used codes are N81.2 for incomplete uterovaginal prolapse, N81.3 for complete uterovaginal prolapse, and N81.4 for unspecified uterovaginal prolapse. This is important because in everyday practice, physicians try to identify not just the general fact of prolapse, but the severity and clinical form. [6]
The International Classification of Diseases, 11th revision, has a more detailed structure. For uterine prolapse, the GC40.3 "Prolapse of the Uterus and Vagina" block is used, within which incomplete prolapse, complete prolapse, and combined variants with anterior and posterior compartments are distinguished. This reflects the current clinical reality: in many patients, not only the uterus but also the anterior or posterior vaginal wall prolapses, so the classification takes into account these combined forms. [7]
In practice, this means that the entry "uterine prolapse" is clear to the patient, but for medical documentation, it is usually clarified. Incomplete prolapse is one situation, complete prolapse, or procidentia, is another. And combined uterine prolapse with cystocele or rectocele is a third, because the symptoms, risks, and surgical approaches in these cases differ. [8]
Table 2. Main codes
| Classification | Code | Meaning |
|---|---|---|
| ICD 10 | N81.2 | Incomplete uterovaginal prolapse |
| ICD 10 | N81.3 | Complete uterovaginal prolapse |
| ICD 10 | N81.4 | Unspecified uterovaginal prolapse |
| ICD 11 | GC40.30 | Incomplete uterovaginal prolapse |
| ICD 11 | GC40.34 | Complete uterovaginal prolapse |
| ICD 11 | GC40.3Z | Uterovaginal prolapse, unspecified |
Sources for the table: [9]
Epidemiology
The exact prevalence of uterine prolapse is difficult to determine because many women do not seek help, especially if the symptoms are mild. However, the problem is very common, especially in older age groups. The Royal College of Obstetricians and Gynaecologists estimates that symptoms of pelvic organ prolapse occur in approximately 1 in 10 women over 50, and mild forms often cause no noticeable symptoms at all. [10]
If we focus not only on symptoms but also on examination data, the range of figures is much wider. A modern review from 2025 indicates that in surveys, the prevalence of symptomatic prolapse can range from 1% to 31%, while in studies with physical examination, signs of prolapse are found in 10%-50% of women, and even more frequently in certain groups. This demonstrates an important point: anatomical prolapse and clinically significant prolapse are not the same thing. [11]
From a public health perspective, the frequency with which prolapse leads to surgery is also important. According to a large study, by age 80, the lifetime risk of requiring surgery for pelvic organ prolapse reaches approximately 12.6%, while earlier estimates for prolapse or urinary incontinence surgery put the figure at approximately 11.8%. This means that surgical treatment is not required for everyone, but the need for it remains high. [12]
Age plays a significant role. Both clinical reviews and population-based studies show that prolapse is more common in older and postmenopausal women. This is due not only to previous childbirth but also to the accumulation of changes in connective tissue, pelvic floor muscles, hormonal levels, and overall mechanical stress on the pelvic diaphragm. [13]
Table 3. What is known about prevalence
| Indicator | What the data shows |
|---|---|
| Symptoms of prolapse in women over 50 | About 1 in 10 |
| Symptomatic prevalence in surveys | Approximately 1% to 31% |
| Prevalence according to examination data | Approximately 10% to 50% |
| Lifetime risk of prolapse surgery by age 80 | About 12.6% |
| The main age group at risk | Older and postmenopausal women |
Sources for the table: [14]
Reasons
Uterine prolapse occurs when the pelvic support system can no longer cope with normal loads. Normally, the uterus and vagina are supported by the pelvic floor muscles, primarily the levator muscles, as well as by ligaments and fascial structures. Modern reviews emphasize that the normal position of the pelvic organs depends on both the muscular support and the connective tissue support of the uterus and vagina. [15]
The most important cause is damage to the pelvic floor during pregnancy and childbirth, especially vaginal. A StatPearls review clearly states that vaginal delivery remains the most significant risk factor, especially in high-parity settings, large fetuses, instrumental deliveries, and prolonged second stages of labor. This is explained by direct trauma to the muscles, fascia, and levator complex. [16]
With age and after menopause, the problem intensifies. Supporting tissues become less elastic, muscles lose strength, and the collagen framework changes. Against this background, even previous damage that was compensated for in youth may begin to manifest clinically. This is why, in many women, prolapse becomes noticeable not immediately after childbirth, but years or decades later. [17]
Additional causes may include obesity, chronic cough, persistent constipation, heavy physical work, congenital weakness of connective tissue, and certain pelvic surgeries. It's also important to note that uterine prolapse is rarely the result of a single event. Rather, it's the result of years of accumulated stress and the gradual depletion of the support system. [18]
Table 4. Main causes of uterine prolapse
| Cause | How does it work? |
|---|---|
| Vaginal birth | Trauma to the muscles and fascia of the pelvic floor |
| Age and menopause | Weakens muscles and connective tissue |
| Obesity | Increases chronic intra-abdominal pressure |
| Chronic constipation | Increases straining and mechanical stress |
| Chronic cough | Increases pressure on the pelvic floor |
| Heavy physical labor | Maintains constant overload |
Sources for the table: [19]
Risk factors
The most consistently confirmed risk factors are age, vaginal delivery, parity, and body mass index. A classic review of prolapse and modern generalizing articles cite these factors as the most consistent and reproducible. In practice, this means that prolapse almost always develops as a result of a combination of obstetric and age-related stress, rather than out of nowhere. [20]
The characteristics of the birth process are particularly important. The risk increases with a large fetus, instrumental delivery, a prolonged second stage of labor, and repeated vaginal deliveries. These circumstances increase the likelihood of damage to the levator muscles and supporting ligaments, which largely determine the future stability of the uterovaginal complex. [21]
Important modifiable factors include obesity, chronic constipation, and heavy lifting. NICE specifically recommends discussing weight loss in patients with a body mass index (BMI) of over 30 kg/m², minimizing heavy lifting, and preventing or treating constipation in those with prolapse. This is a good example of how guidelines translate pathophysiology into specific everyday advice. [22]
Finally, individual predisposition also plays a role. Some women have family and connective tissue vulnerabilities, which can lead to prolapse developing more rapidly and with less obstetric stress. Modern reviews increasingly view prolapse as the result of a combination of mechanical trauma, hormonal influences, and genetically determined connective tissue quality. [23]
Table 5. Main risk factors
| Factor | Degree of clinical importance |
|---|---|
| Age | High |
| Multiple vaginal births | High |
| Large fetus and instrumental delivery | High |
| Obesity | High |
| Chronic constipation and straining | High |
| Chronic cough | Moderate and high |
| Family predisposition | Probably significant |
Sources for the table: [24]
Pathogenesis
The pathogenesis of uterine prolapse is associated with a disruption of the balance between load and support. As long as the pelvic floor muscles, fascia, and ligaments support intra-abdominal pressure, the uterus maintains its normal position. When muscular support weakens and the connective tissue becomes weaker, the apex of the vagina and the uterus begin to shift downward. Modern reviews describe this process as a combination of damage to the levator muscle and disruption of the connections of the pelvic organs to the pelvic lateral wall. [25]
The apical support structures, primarily the cardinal and uterosacral ligaments, are particularly important for uterine prolapse. When these ligaments lengthen, weaken, or fail to withstand the load, the uterus loses its primary apical support. In this case, both the midline and distal support structures are often affected simultaneously, which is why isolated uterine prolapse is often combined with cystocele or rectocele. [26]
At the cellular level, collagen remodeling, extracellular matrix changes, connective tissue cell apoptosis, and impaired soft tissue repair after birth trauma are discussed. These mechanisms have been particularly actively studied in recent years because they help explain why some women do not develop prolapse after multiple births, while others experience it relatively early. [27]
This is why uterine prolapse cannot be explained simply by "weak muscles." The actual process is more complex: it is a combined failure of the muscular, ligamentous, and fascial support due to chronic strain. This understanding is also important for treatment, as it explains why some women respond to exercise and a pessary, while others require surgical restoration of the apical support. [28]
Table 6. How uterine prolapse develops
| Stage | What's happening |
|---|---|
| 1 | Pelvic floor muscles and connective tissue are damaged |
| 2 | The apical support of the uterus and vagina weakens |
| 3 | The uterus begins to shift downwards under load and straining |
| 4 | Symptoms of pressure, bulging and urinary problems appear. |
| 5 | As the condition progresses, the uterus may partially or completely extend beyond the vagina. |
Sources for the table: [29]
Symptoms
The most characteristic symptom is the sensation of a bulge, a foreign body, or a "ball" in the vagina. Many women describe this as a feeling of heaviness, a pulling pressure, or something protruding outward, which intensifies in the evening, after prolonged standing and physical activity, and subsides when lying down. These complaints are most typical of clinically significant prolapse. [30]
Urinary symptoms are no less common. A woman may complain of increased frequency of urination, urgency, difficulty initiating urination, a feeling of incomplete bladder emptying, stress urinary incontinence, or recurrent urinary tract infections. With severe prolapse, some symptoms may even be masked, and this is important to consider before treatment. [31]
Bowel symptoms may include constipation, a feeling of incomplete evacuation, the need to strain, and sometimes the need to press on the protrusion with a finger to facilitate defecation. Such complaints are especially common in cases of uterine prolapse combined with posterior prolapse. Clinical guidelines consider an assessment of bowel function a mandatory part of the initial examination. [32]
Sexual function can also change. Discomfort, a feeling of obstruction, decreased sensitivity, fear of intercourse, and severe psychological inhibition are all possible. However, in some women, prolapse remains asymptomatic for a long time, especially in the early stages. This explains why the degree of anatomical prolapse does not always correspond to the severity of complaints. [33]
Table 7. The most common symptoms
| Symptom | How does it feel? |
|---|---|
| Bulge in the vagina | Feeling of a "ball", foreign body, or tissue falling out |
| Pelvic heaviness | Pressure, pulling sensation, discomfort |
| Urination disorder | Frequent urges, incomplete emptying, leakage |
| Intestinal symptoms | Constipation, straining, feeling of incomplete evacuation |
| Sexual discomfort | Pain, fear, feeling of obstacle |
| Asymptomatic course | Early stage without noticeable complaints is possible |
Sources for the table: [34]
Classification, forms and stages
Clinically, uterine prolapse is divided into incomplete and complete. In incomplete prolapse, the uterus descends but does not protrude completely. In complete prolapse, or procidentia, the uterus may be located entirely outside the vagina. This distinction is reflected in both the International Classification of Diseases, 10th revision, and the International Classification of Diseases, 11th revision. [35]
For objective assessment, a quantitative pelvic organ prolapse assessment system is now internationally accepted. NICE recommends using this system for specialized assessments, recording the degree of prolapse of the anterior, central, and posterior compartments. This system is useful not only for science but also for practice, as it helps to consistently describe prolapse before and after treatment. [36]
The stages in this system are designated from 0 to 4. Stage 0 means no prolapse. Stage 1 means the most distal part of the prolapse is located more than 1 cm above the level of the hymen. Stage 2 means the prolapse is within 1 cm above or below the hymen. Stage 3 means the prolapse extends more than 1 cm below the hymen, but does not reach complete eversion. Stage 4 means almost complete eversion. [37]
It's also important to note that uterine prolapse is often not isolated. In practice, the physician simultaneously evaluates the central, anterior, and posterior compartments of the pelvic floor. Therefore, a woman may be diagnosed not only with uterine prolapse but also with combined uterine prolapse with a cystocele or rectocele. This description is more accurate and useful for treatment selection. [38]
Table 8. Stages of uterine prolapse according to the modern system
| Stage | What does this mean? |
|---|---|
| 0 | There is no prolapse |
| 1 | The lowest point is more than 1 cm above the hymen |
| 2 | The lowest point within 1 cm above or below the hymen |
| 3 | Prolapse more than 1 cm below the hymen, but without complete eversion |
| 4 | Almost complete prolapse and eversion |
Sources for the table: [39]
Complications and consequences
Although uterine prolapse is usually not life-threatening, complications are quite real. Primarily, these include urinary dysfunction, including residual urine, urinary tract infections, and combined incontinence. With severe prolapse, urinary symptoms may either worsen or be masked, so they must be assessed separately, sometimes after the prolapse has been reduced during examination. [40]
Intestinal complications include persistent constipation, difficult defecation, and, in rare, severe cases, even intestinal obstruction. Statistically, this is not the most common complication, but clinically it is very important, especially in posterior prolapse and severe combined prolapse. Patients often describe the need to use a finger to assist with bowel movements, and this symptom should not be underestimated. [41]
With prolonged, severe prolapse, irritation of the mucous membrane, ulceration, contact bleeding, and trauma to the prolapsed tissue are possible. This is especially likely with complete prolapse, when the tissues constantly rub against underwear and are exposed to external influences. In postmenopausal women, mucous membrane atrophy further increases vulnerability. [42]
Finally, the psychological consequences cannot be underestimated. Prolapse can dramatically reduce self-confidence, limit physical activity, disrupt sexual function, and lead to social isolation. Therefore, uterine prolapse is not only an anatomical problem, but also a disruption of daily function and quality of life. [43]
Table 9. Main complications
| Complication | What could be happening? |
|---|---|
| Urination disorder | Residual urine, infections, incontinence |
| Constipation and difficult bowel movements | Straining, incomplete emptying |
| Traumatization of the mucous membrane | Ulceration, irritation, bloody discharge |
| Pain and discomfort | Increased in the evening and with exercise |
| Sexual dysfunction | Discomfort, fear, decreased quality of life |
| Psychological distress | Shame, anxiety, social restriction |
Sources for the table: [44]
When to see a doctor
You should consult a doctor immediately if you experience a sensation of a bulge in the vagina, a pulling sensation, or visible tissue prolapse. This doesn't necessarily mean surgery is needed immediately, but such symptoms warrant an examination, as early assessment can determine the choice of a more gentle treatment. NICE recommends that if a prolapse is symptomatic or accidentally discovered, a detailed medical history be taken, an examination performed, and the woman's preferences discussed at the initial contact. [45]
Urinary difficulties, recurrent urinary tract infections, inability to completely empty the bladder, severe constipation, pain, bloody discharge from prolapsed tissue, or a rapid worsening of symptoms require immediate medical attention. These signs may indicate not just a mild prolapse, but a clinically significant pelvic organ dysfunction. [46]
Women whose prolapse interferes with walking, sitting, working, physical activity, or sexual activity require special attention. Current guidelines emphasize that treatment is indicated when the prolapse is truly bothersome and disrupts function. Therefore, the criterion for seeking treatment is not only the size of the prolapse but also the degree of everyday and sexual discomfort. [47]
Table 10. Situations when an in-person assessment is needed
| Situation | How urgent is this? |
|---|---|
| A feeling of bulging or heaviness | Scheduled consultation |
| Visible tissue loss | Scheduled and expedited consultations |
| Difficulty urinating | Quick consultation |
| Frequent urinary tract infections | Quick consultation |
| Bloody discharge, ulcers, pain | Quick consultation |
| Severe impairment of quality of life | Mandatory discussion of treatment |
Sources for the table: [48]
Diagnostics
Diagnosis of uterine prolapse in most cases begins with a consultation and a routine gynaecological examination. NICE recommends taking a medical history at the initial consultation, including an assessment of prolapse symptoms, urinary function, bowel function, and sexual function. This is important because two women with the same stage of prolapse may present with significantly different symptoms. [49]
During the examination, the physician must not only detect the protrusion but also rule out a pelvic tumor or other pathology. A specialized assessment uses a standard quantitative pelvic organ prolapse assessment system, evaluates pelvic floor muscle activity and the condition of the vaginal mucosa, including signs of atrophy. If the prolapse appears less pronounced in the supine position, the examination may be repeated while standing or straining. [50]
Imaging is not usually necessary to confirm a visible prolapse. NICE specifically states that imaging should not be routinely performed to document a prolapse detected on physical examination. The Irish National Clinical Guideline also notes that pelvic floor ultrasound is not usually required for diagnosis in uncomplicated mesh implants. [51]
However, additional investigations are needed when complaints extend beyond simple anatomy. For urinary symptoms, residual urine is assessed, urinalysis is performed, and, if necessary, urodynamic studies are performed. In cases of severe intestinal complaints, pain, or a discrepancy between symptoms and examination, the examination is expanded. This approach allows for the treatment of not only "visual prolapse," but also the actual functional problem of the individual patient. [52]
Table 11. Step-by-step diagnostics
| Stage | What are they doing? | For what |
|---|---|---|
| 1 | Detailed survey | Assess complaints, urinary, intestinal and sexual function |
| 2 | Gynecological examination | Confirm the presence of prolapse |
| 3 | Examination during straining and, if necessary, while standing | See the maximum omission |
| 4 | Standardized stage assessment | Record the degree of prolapse |
| 5 | Assessment of the pelvic floor muscles and mucosa | Plan treatment |
| 6 | Additional tests if indicated | Clarify urinary and intestinal disorders |
Sources for the table: [53]
Differential diagnosis
At the first level, the doctor needs to understand what exactly is prolapsed. A woman may say "the uterus is prolapsing," but upon examination, the main problem sometimes turns out to be an anterior prolapse with bladder protrusion, a posterior prolapse involving the rectum, or a prolapse of the apex of the vagina after a previous hysterectomy. This is why modern diagnostics require describing the anterior, central, and posterior compartments separately. [54]
The second important step is to rule out a pelvic tumor and other pathologies that could mimic or be associated with prolapse. NICE specifically recommends that the initial assessment be conducted to rule out pelvic masses and other pathologies. This is especially important in cases of atypical complaints, pain, rapid worsening of symptoms, or clinical findings inconsistent with typical prolapse. [55]
It is also important to distinguish between anatomical prolapse and functional disorders, which can cause similar symptoms. For example, a feeling of heaviness and difficulty urinating may be associated with an overactive bladder, incomplete bladder emptying for another reason, or functional bowel dysfunction. Therefore, a good diagnosis of uterine prolapse always includes an assessment of not only the form but also the function. [56]
Table 12. What should be distinguished from uterine prolapse?
| State | What is the difference? |
|---|---|
| Anterior prolapse | The protrusion of the anterior vaginal wall and urinary symptoms are dominant. |
| Posterior prolapse | Constipation and difficulty with defecation are more common. |
| Prolapse of the vaginal apex after hysterectomy | The uterus is no longer there, but the top of the vagina is lowered |
| Pelvic tumor or other mass | May cause a feeling of pressure without the typical picture of prolapse |
| Functional urinary and intestinal disorders | Complaints may be more pronounced than anatomical changes |
Sources for the table: [57]
Treatment
Treatment for uterine prolapse begins not with surgery, but with a discussion of goals. NICE recommends discussing the option of no treatment, non-surgical methods, and surgical solutions with the woman, taking into account her preferences, prolapse type, age, comorbidities, previous surgeries, and childbearing plans. This is an important modern principle: treatment should be tailored to the woman's life, not to a pretty plan on paper. [58]
If symptoms are minimal and the woman does not want active treatment, observation is acceptable. The Irish National Clinical Guidelines explicitly state that symptom monitoring is a reasonable option if the patient is comfortable with this approach. This is especially important for mild cases, in which anatomical prolapse is present but there is no significant discomfort. [59]
The first non-surgical step is lifestyle changes. NICE recommends discussing weight loss if obese, minimizing heavy lifting, and preventing or treating constipation. These measures do not "re-elevate" the uterus, but they reduce the constant mechanical stress on the pelvic floor and can reduce symptoms and slow further deterioration. [60]
Pelvic floor muscle training plays a special role. NICE recommends a course of supervised exercise for at least 16 weeks as the first treatment option for women with symptomatic stage 1 and 2 prolapse. National guidelines in Ireland recommend the same approach and recommend continuing the exercises after achieving benefits. This is one of the few conservative treatments that can actually reduce symptoms in some patients. [61]
If a woman has signs of genitourinary syndrome of menopause, topical vaginal oestrogen may help. NICE recommends considering it in women with prolapse and menopausal urogenital symptoms. This medication does not correct the prolapse itself, but it can reduce dryness, irritation, discomfort, and improve pessary tolerability. [62]
A very important non-surgical method is the vaginal pessary. NICE recommends considering it in women with symptomatic prolapse, either alone or in conjunction with pelvic floor muscle training. The pessary is suitable for many patients, including those who wish to delay surgery, preserve fertility, or have a high surgical risk. A review by the US National Institutes of Health also emphasizes that exercises and pessaries often provide sufficient symptom relief. [63]
The pessary requires selection and monitoring. The Irish guidelines note that if a standard ring pessary is not suitable, other designs, such as the Gellhorn type, can be considered. If the woman is unable to remove and insert the pessary independently, regular checkups are necessary approximately every 3-6 months; if she is able, at least annual monitoring is recommended. In case of mucosal erosion, temporary removal of the pessary, topical estrogen, and, if necessary, antimicrobial treatment are standard considerations. [64]
Surgical treatment is considered when symptoms are severe, conservative methods have failed or are unsuitable, and the woman desires a more radical solution. NICE recommends separate discussion of complications and the limitations of long-term data, as well as the use of shared decision-making tools, for uterine prolapse surgery. In other words, modern prolapse surgery involves not only surgical technique but also a high-quality preoperative discussion. [65]
If a woman does not insist on preserving the uterus, NICE offers a choice between vaginal hysterectomy with or without fixation, vaginal sacrospinous hysteropexy, the Manchester procedure, and sacrohysteropexy with mesh material via an abdominal or laparoscopic approach. If a woman wishes to preserve the uterus, NICE suggests sacrospinous hysteropexy, the Manchester procedure, and sacrohysteropexy via an abdominal or laparoscopic approach. Current evidence from 2025 also supports laparoscopic hysteropexy as a viable organ-preserving alternative for apical prolapse. [66]
For older women who do not plan to have vaginal intercourse and who are at high risk of complications, NICE recommends colpocleisis. This is an obliterative procedure that does not preserve the vaginal opening for penetrative sex but is less invasive. The Irish National Clinical Guidelines also consider obliterative procedures a reasonable option for older, medically compromised, and sexually inactive patients. [67]
Mesh material deserves special consideration. NICE recommends that transvaginal polypropylene mesh procedures for anterior and posterior prolapse should only be used in research settings due to serious safety concerns and a lack of data on long-term effectiveness. This is a very important current finding, as mesh technologies in prolapse surgery have generated the most regulatory restrictions and controversy. [68]
Table 13. Modern treatment methods
| Method | When it suits | What does it give? |
|---|---|---|
| Observation | For mild symptoms | Avoiding unnecessary treatment |
| Lifestyle changes | Almost everyone | Reducing stress on the pelvic floor |
| Pelvic floor muscle training | Symptomatic prolapse stages 1 and 2 | Reduction of symptoms |
| Vaginal estrogen | For menopausal atrophy | Improving fabric comfort |
| Pessary | In case of symptomatic prolapse, unwillingness or impossibility of surgery | Mechanical support |
| Vaginal hysterectomy | In case of uterine prolapse without the goal of preserving the uterus | Radical elimination of central prolapse |
| Hysteropexy | If you want to keep the uterus | Organ-preserving surgical treatment |
| Colpocleisis | If there is a high risk of surgery and you refuse penetrative sex | Reliable reduction of prolapse with low load |
| Transvaginal mesh | Not recommended for routine use outside of research studies. | Limited due to security concerns |
Sources for the table: [69]
Prevention
Preventing uterine prolapse does not guarantee complete protection, but it can reduce the risk and delay the onset of symptoms. NICE 2021 recommends encouraging women of all ages to practice pelvic floor muscles and to continue this throughout their lives, as long-term practice helps prevent symptoms of pelvic floor dysfunction. This is one of the most practical and realistic preventative strategies. [70]
Equally important are weight management, avoiding chronic heavy lifting, and preventing constipation. NICE 2019 explicitly includes these points in its lifestyle recommendations for prolapse. Even if prolapse has already occurred, such correction reduces its progression and reduces the daily strain on the pelvic floor. [71]
Prevention is especially important after childbirth and during perimenopause. It is during these periods that a woman can either ignore the first signs of pelvic floor weakness or begin training and correcting risk factors promptly. Current data shows that prolapse often progresses slowly, and in some women, symptoms may remain stable or even partially improve. Therefore, prevention and early attention to symptoms are truly valuable. [72]
Table 14. What helps in prevention
| Measure | Why is it useful? |
|---|---|
| Regular pelvic floor muscle training | Supports muscular support of organs |
| Weight control | Reduces intra-abdominal pressure |
| Prevention of constipation | Reduces straining |
| Limit heavy lifting | Reduces chronic overload |
| Chronic cough control | Reduces repetitive strain on the pelvic floor |
| Early treatment at the first symptoms | Allows you to start gentle treatment earlier |
Sources for the table: [73]
Forecast
The prognosis for uterine prolapse is generally favorable, meaning the condition is usually not life-threatening. However, the prognosis for quality of life depends heavily on the severity of symptoms, associated urinary and intestinal disorders, age, and the chosen treatment strategy. In some women, symptoms remain stable for a long time, in others they gradually worsen, and in others they improve after conservative measures. [74]
With conservative treatment, a significant proportion of women experience significant relief. The US National Institutes of Health indicates that for many, exercise and a pessary are sufficient to reduce prolapse symptoms. With surgical treatment, StatPearls reports high rates of symptomatic improvement and patient satisfaction, although the risk of recurrence and retreatment remains. [75]
It's crucial to understand that anatomical and subjective results don't always align. Even with a good anatomical result, a woman's primary concern is whether the bulging sensation has disappeared, whether urination has become easier, whether constipation has resolved, and whether life has become more comfortable. This is why modern societies increasingly emphasize the importance of not only staging prolapse but also considering patient outcomes and quality of life. [76]
Table 15. What the forecast depends on
| Factor | Impact on outcome |
|---|---|
| Stage of prolapse | The higher the stage, the more often active measures are needed. |
| Severity of symptoms | Determines the real impact on quality of life |
| Associated urinary and intestinal disorders | May impair daily function |
| Answer to the pessary and exercises | For some women, it allows them to go a long time without surgery. |
| Type of surgery and technique | Affect the risk of relapse and satisfaction |
| Lifetime stress factors | Obesity, constipation and heavy work increase the risk of deterioration |
Sources for the table: [77]
FAQ
Are uterine prolapse and uterine prolapse the same thing?
In everyday speech, these terms are often used interchangeably. Clinically, prolapse typically describes earlier forms of uterine downward displacement, while uterine prolapse refers to more advanced stages, especially when tissues reach the vaginal opening or extend beyond it. [78]
Is surgery always necessary for uterine prolapse?
No. If symptoms are moderate or mild, observation, lifestyle changes, pelvic floor exercises, or a pessary can help. Surgery is usually considered when prolapse is truly interfering with life or conservative treatments are ineffective. [79]
Do exercises help lift the uterus back up?
Exercises don't "return" the uterus to its original position like a mechanical operation, but in stages 1 and 2, they can reduce symptoms and improve pelvic floor function. This is why they are recommended as a first step for women with mild to moderate symptomatic prolapse. [80]
What is a pessary and can you live with it long-term?
A pessary is a vaginal support device that helps keep the organs in a more comfortable position. For many women, it works long-term and allows them to delay or avoid surgery altogether, but it requires proper selection and regular monitoring. [81]
Is it possible to preserve the uterus during surgery?
Yes. Current recommendations recommend organ-preserving options, including sacrospinous hysteropexy, the Manchester procedure, and sacrohysteropexy via an abdominal or laparoscopic approach. The choice depends on the woman's anatomy, pregnancy plans, age, and preferences. [82]
What if the bulge only appears in the evening?
This is a typical situation for prolapse. Even if there are few symptoms in the morning, they may intensify in the evening due to gravity and tissue fatigue. In such cases, it is sometimes useful to repeat the examination after straining or while standing, if the prolapse is less pronounced in a normal position than the patient complains of. [83]
Is mesh dangerous in prolapse surgery?
Current guidelines are very cautious about transvaginal polypropylene mesh for anterior and posterior prolapse. NICE states that due to serious safety concerns and weak long-term data, this approach should only be used in research studies. [84]
Can prolapse return after treatment?
Yes, this is a possibility, both after conservative therapy and after surgery. Therefore, it is important not only to choose a treatment but also to continue long-term measures that reduce stress on the pelvic floor. [85]
Key points from experts
Ingrid Nygård, MD, MS, EP, is a professor of obstetrics and gynecology at the University of Utah and a former president of the American Urogynecological Society. Her research consistently emphasizes that pelvic organ prolapse is not just an anatomy issue but also a woman's actual quality of life. The practical implication of this approach is simple: it's not just the "stage at examination" that needs to be treated, but the symptoms, function, and extent of prolapse's impact on daily life. [86]
Christopher Maher, Professor of Urogynecology at the University of Queensland, leads international reviews of surgical treatment for prolapse. His key practical thesis is that prolapse surgery should be evidence-based and individualized. In the context of uterine prolapse, this is especially important, because today women should be given a real choice between hysterectomy, uterine-preserving surgery, and non-surgical options, not just a single, standardized scenario. [87]
Marie Fidela Paraiso, MD, a specialist in pelvic floor medicine and reconstructive surgery at the Cleveland Clinic, reflects the current understanding of the problem: good prolapse surgical outcomes depend on a precise anatomical understanding, minimally invasive skills, and the ability to combine functional and reconstructive goals. For the patient, this means that in cases of severe uterine prolapse, the quality of the center and the surgeon's experience truly matter. [88]
Conclusion
Uterine prolapse is a common condition that most often develops as a result of birth trauma, age-related changes, and prolonged pelvic floor strain. It is rarely life-threatening, but can seriously interfere with urination, defecation, sexual function, and physical well-being. The main advantage of modern medicine in this area is that there is now not just one, but several effective treatment options: observation, exercises, pessaries, organ-preserving surgeries, and hysterectomy. [89]