Medical expert of the article

New publications
Symptoms of Minkowski-Schoffar disease.
Last reviewed: 06.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
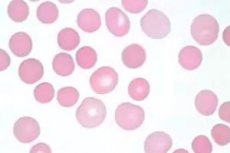
Hereditary microspherocytosis is clinically manifested in 50% of cases already in the neonatal period; in the vast majority of patients, the disease begins before adolescence. It has been established that the early appearance of symptoms of the disease predetermines a more severe course.
The central place in the clinical picture is occupied by three leading symptoms caused by the intracellular localization of hemolysis: jaundice, pallor of the skin and mucous membranes, splenomegaly.
The intensity of jaundice may vary and is determined by the level of indirect bilirubin. In some patients, icterus of the skin and sclera may be the only symptom for which they seek medical attention. It is to these patients that the famous expression of Chauffard applies: "they are more jaundiced than sick." A distinctive feature of jaundice is its acholuricity, that is, the absence of bile pigments in the urine, but urobilinuria is noted.
The pallor of the skin and mucous membranes is caused by the presence of anemia and its severity depends on the degree of anemia; outside of a hemolytic crisis, the pallor is less pronounced, but during a crisis it is sharp.
The degree of splenomegaly is variable; at the height of the crisis, the spleen is significantly enlarged, dense, smooth, and painful upon palpation. There is an enlarged liver. During the compensation period, splenomegaly persists, but is expressed to a lesser degree.
Children aged 4-5 years often have gallstones, but cholelithiasis is most often diagnosed in adolescents. Cholelithiasis occurs in approximately 50% of patients who have not undergone splenectomy.
Patients often have a tower skull, gothic palate, wide nasal bridge, dental anomalies, syndactyly, polydactyly, heterochromia of the iris. In severe, progressive cases of the disease, growth retardation, mental retardation, and hypogenitalism are possible.
Depending on the severity, three forms of the disease are distinguished. In the mild form, the general condition is satisfactory, hemolysis and splenomegaly are expressed insignificantly. In the moderate form, mild or moderate anemia with uncompensated hemolysis and episodes of jaundice, pronounced splenomegaly are observed. In the severe form, pronounced anemia is observed, which requires repeated blood transfusions, aregenerative crises may occur, and growth retardation is observed.
Classification of hereditary spherocytosis and indications for splenectomy
Signs |
Norm |
Classification of spherocytosis |
||
Easy |
Moderate severity |
Heavy |
||
Hemoglobin (g/l) |
110-160 |
110-150 |
80-120 |
60-80 |
Reticulocyte count (%) |
<3 |
3.1-6 |
>6 |
>10 |
Reticulocyte index |
<1.8 |
1.8-3 |
>3 |
|
Spectrin content in erythrocytes (in % of normal) 2 |
100 |
80-100 |
50-80 |
40-60 |
Osmotic resistance |
Norm |
Normal or slightly reduced |
Sharply reduced |
Sharply reduced |
Autohemolysis without glucose (%) in the presence of glucose |
>60 <10 |
>60 >10 |
0-80 > 10 |
50 >10 |
Splenectomy |
Usually there is no need |
Must be completed before puberty |
Shown, better to perform after 3 years |
|
Clinical symptoms |
None |
Pallor, aregenerative crisis, splenomegaly, cholelithiasis |
Pallor, aregenerative crisis, splenomegaly, cholelithiasis |
|
Aregenerator crisis is a severe complication of hemolytic crisis, during which symptoms of bone marrow hypoplasia with selective damage to the erythroid germ appear. It is believed that the development of aregenerator crisis, as a rule, is caused by the addition of a viral infection caused by parvovirus B19. Aregenerator states of the bone marrow last from several days to 2 weeks, cause severe anemia and can be the main cause of death of the patient. Clinically, pronounced pallor of the skin and mucous membranes is observed in the complete absence of icterus of the skin and sclera, an increase in the spleen is absent or expressed insignificantly and there is no correspondence between the severity of splenomegaly and the severity of the anemic crisis. Reticulocytosis is absent, up to the complete disappearance of reticulocytes from the peripheral blood. Thrombocytopenia is detected in some children. Aregenerative crises are observed mainly in children aged 3-11 years and, despite their severity, are reversible.
The course of Minkowski-Chauffard anemia is undulating; following the development of a crisis, clinical and laboratory parameters improve and remission occurs, lasting from several months to several years.
Complications
Hemolytic crisis is a sharp increase in hemolysis processes, often against the background of infection.
Erythroblastopenic (aplastic) crisis - arrest of maturation of erythroid cells - is often associated with megaloblastic changes. It is usually provoked by parvovirus B19 infection, since parvovirus B19 affects developing normoblasts, causing a transient cessation of their production.
Folate deficiency due to accelerated red blood cell turnover can lead to the development of severe megaloblastic anemia.
Gallstone disease occurs in approximately half of untreated patients, and the likelihood of its development increases with age.
Secondary iron overload is rare.
 [ 1 ]
[ 1 ]