Medical expert of the article

New publications
Strabismus - Surgery
Last reviewed: 06.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The goal of strabismus surgery on the extraocular muscles is to achieve correct eye positioning and, if possible, restore binocular vision. However, the first step in treating childhood strabismus is to correct any significant refractive errors and/or amblyopia.
Once the maximum possible visual functions have been achieved in both eyes, any residual deviation must be surgically corrected. There are 3 main operations for strabismus: weakening, reducing the force of traction, strengthening, increasing the force of traction, changing the direction of muscle action.
 [
[ Strabismus: operations that weaken the action of the muscle
There are 3 types of surgeries that weaken the action of the muscle: recession, myectomy, posterior fixation sutures.
Recession
This is a weakening of a muscle by moving its insertion posteriorly toward the origin of the muscle. Recession can be performed on any muscle except the superior oblique.
Rectus recession
- After exposure of the muscle, two absorbable sutures are placed on the outer quarter of the tendon width;
- the tendon is cut from the sclera, the size of the recession is measured and marked on the sclera with a caliper;
- The stump is sutured to the sclera posterior to the original attachment site.
Inferior oblique muscle recession
- exposure of the muscle belly is achieved through an inferotemporal arcuate incision;
- one or two absorbable sutures are placed on the muscle near its attachment site;
- The muscle is cut off, and the stump is sutured to the sclera 2 mm from the temporal edge (the attachment site of the inferior rectus muscle).
Strabismus: myectomy surgery
The procedure involves cutting the muscle at its attachment without reattaching it. This technique is most often used to relieve hyperfunction of the inferior oblique muscle. This intervention is very rarely performed on the rectus muscles when the muscle is highly contracted.
Strabismus: posterior fixation suture operation
The principle of this intervention (Faden operation) is to reduce the strength of the muscles in their direction of action without changing the site of insertion. The Faden operation can be used for VDD, as well as for weakening the horizontal rectus muscles. When correcting VDD, the superior rectus muscle is usually recessed first. The belly of the muscle is then sutured to the sclera with a non-absorbable thread at a distance of 12 mm posterior to its insertion.
Strabismus: operations that enhance the action of the muscle
- Resection of the muscle increases its effective traction. This procedure is suitable only for the rectus muscles and includes the following interventions:
- a) after exposure of the muscle, two absorbable sutures are passed through the muscle at the marked points behind the site of its attachment;
- b) the part of the muscle in front of the sutures is excised, and the stump is sutured to the original attachment site;
- Formation of a muscle or tendon fold is usually used to enhance the action of the superior oblique muscle in congenital paresis of the fourth pair of cranial nerves.
- Repositioning (suturing the muscle closer to the limbus) may provide increased action following previous rectus recession.
Treatment of paralytic strabismus
Paralysis of the external rectus muscle
Surgical intervention for paralysis of the sixth pair of cranial nerves should be performed only in cases where spontaneous improvement does not occur, which can be judged no earlier than after 6 months. There are 2 main interventions that improve abduction:
Operation Hummelsheim
- recession of the internal rectus muscle;
- The lateral halves of the superior and inferior rectus muscles are cut off and sutured to the superior and inferior edges of the paretic lateral rectus muscles.
Since all three muscles are separated from the eyeball during this procedure, there is a risk of postoperative anterior segment ischemia. To avoid this complication, recession of the internal rectus muscle can be replaced by chemodenervation with CI botulinum toxin.
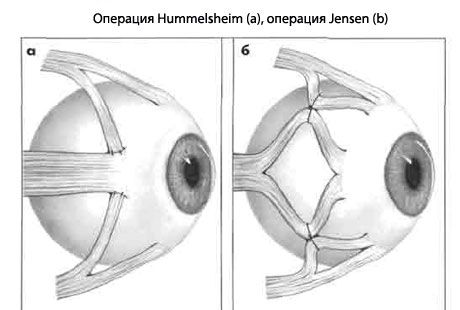
The Jensen procedure improves abduction and is combined with recession or with injection of CI botulinum toxin into the lateral rectus muscle.
- the superior, lateral and inferior rectus muscles are split lengthwise;
- Using non-absorbable sutures, the outer half of the superior rectus muscle is fixed to the upper half of the lateral rectus, and the lower half of the lateral rectus is fixed to the outer half of the inferior rectus.
Superior oblique muscle paralysis
Surgical intervention is indicated in cases of forced head position and diplopia that cannot be corrected with prisms.
- Congenital hypertropia with a large angle in the primary position. In this case, a fold of the superior oblique muscle is performed.
- Acquired
- small hypertropias are corrected by ipsilateral weakening of the inferior oblique muscle;
- Acquired hypertropias with medium and large angles are eliminated by ipsilateral weakening of the inferior oblique muscle, combined with ipsilateral weakening of the superior rectus and/or contralateral weakening of the superior rectus muscle. It should be taken into account that weakening of the inferior oblique and superior rectus muscles of the same eye can lead to hyperelevation;
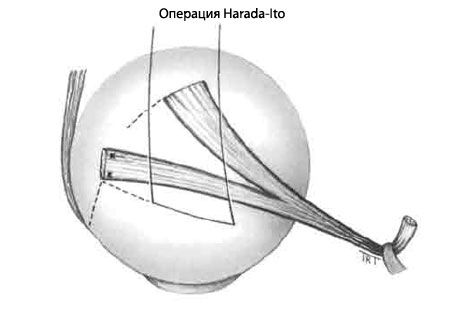
- Excyclotropia without hypertropia is corrected by the Harada-Ito operation, which includes splitting and anterolateral transposition of the outer half of the superior oblique tendon.
Strabismus: adjustable stitches
Indications
In some cases, the best surgical results are achieved with adjustable sutures. Special indications include the need for correct eye positioning and cases where the results of traditional interventions are difficult to predict. For example, acquired vertical deviations in endocrine myopathy or consequences of an impacted orbital floor fracture. Other relative indications include paralysis of the sixth pair of cranial nerves, exotropia in adults, and repeated surgeries with scarring of surrounding tissues, when the result of the operation may be unpredictable. The main contraindication is the patient's young age or the impossibility of postoperative suture adjustment.
The first stages
- The muscle is exposed, sutures are applied, the tendon is separated from the sclera (as in rectus muscle recession).
- The two ends of the thread are passed close together through the stump at the point of attachment.
- The second suture is tied and pulled tightly around the muscle suture at the front to secure it from the stump.
- One end of the seam is cut off and the two ends are tied together to form a loop.
- The conjunctiva remains open.
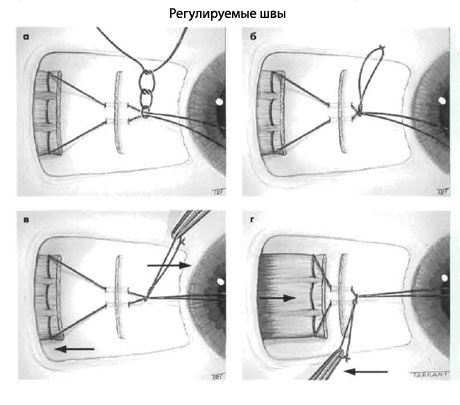
Postoperative regulation
- Assess the position of the eyes.
- If the position of the eyes is satisfactory, the muscle suture is tied and the long ends of the thread are shortened.
- If a larger recession is required, the knot is pulled anteriorly along the muscle suture, providing additional relaxation of the recessed muscle, and pushed posteriorly.
- If less recession is required, the muscle suture is pulled forward and the knot is pulled in the direction opposite to the muscle stump.
- The conjunctiva is sutured.
A similar technique is used for resection of the rectus muscle.
Strabismus: chemodenervation with CI botulinum toxin
Temporary paralysis of the extraocular muscle can be created in addition to the transposition described earlier, or in isolation. The main indications for chemodenervation are:
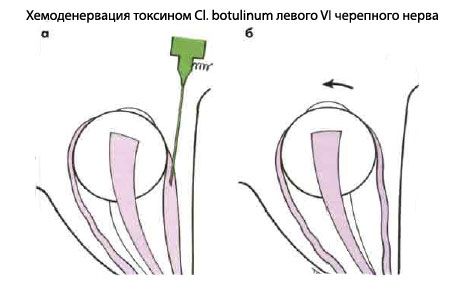
- To determine the function of the external rectus muscle in paralysis of the sixth pair of cranial nerves, in which contracture of the internal rectus muscle interferes with abduction, a small dose of CI toxin botulinum is injected into the belly of the antagonist in hyperfunction (internal rectus muscle) under electromyographic control. Temporary paralysis of the muscle causes its relaxation, and the action of the horizontal muscles of the eye is balanced, allowing the function of the external rectus muscle to be assessed.
- To determine the risk of postoperative diplopia and to assess the potential for binocular vision. For example, in an adult patient with left divergent strabismus and high visual acuity in both eyes, an injection of CI botulinum toxin into the lateral rectus muscle of the left eye will result in either eye alignment or convergence.
However, placing a corrective prism in front of the deviated eye is often a simpler and more accurate method of assessing the risk of postoperative diplopia. If one of the methods indicates the possibility of diplopia, the patient can be advised of this. However, such diplopia usually resolves spontaneously.