Medical expert of the article

New publications
Spleen abscess
Last reviewed: 29.06.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The formation of an encapsulated cavity in the spleen parenchyma filled with purulent exudate is defined as a spleen abscess (from Latin abscessus - pustule, abscess).
Epidemiology
Splenic abscess is a rare disease (its incidence ranges from 0.2% to 0.07%); about 70% of cases develop in patients with concomitant infections; in infective endocarditis, in less than 2% of patients. [1]
Polymicrobial abscesses account for more than 50% of cases, and fungal abscesses account for 7% to 25% of cases.
In adults, about two-thirds of spleen abscesses are solitary (single-chamber) and one-third are multiple (multichamber).
Causes of the spleen abscess
Abscess of the spleen, a peripheral organ of the immune system and extramedullary hematopoiesis, results from inflammation of its tissues, the causes of which may be:
- Presence of bacteria in the blood - bacteremia (caused by chronic infections of various systems and organs, including urinary tract and gastrointestinal tract);
- Septic (infectious) infarction of the spleen with disruption of its blood supply, leading to ischemia (oxygen starvation) of part of the tissues and their necrosis;
- Parasitic infection of the spleen - with infection and suppuration of echinococcal cyst of the spleen (formed by infection with the tapeworm parasite Echinococcus granulosus);
- Subacute infective endocarditis strepto- or staphylococcal origin (abscess is a complication in almost 5% of patients with bacterial inflammation of the inner lining of the heart);
- Typhoid fever, caused by the bacteria Salmonella typhi;
- A systemic zoonotic infectious disease caused by gram-negative bacilli of the Brucellaceae family - brucellosis;
- Spread of infection from neighboring abdominal organs, for example, from the inflamed pancreas in acute pancreatitis (etiologically associated with bacterial infection or parasitic invasion) or inflammation of the pancreatic peritoneal membrane with involvement of the spleen gate.
Spleen abscess can be polymicrobial as well as fungal, caused by Candida species (most commonly Candida albicans). [2]
Risk factors
Factors that increase the risk of spleen abscesses are blunt trauma to the spleen; diabetes mellitus and extrapulmonary forms of tuberculosis; [3] autoimmune hemolytic anemia and such chronic hemoglobinopathies as sickle cell anemia (with structural changes in red blood cells); immune weakening - immunosuppression [4] (including HIV); Felty's syndrome (a form of rheumatoid arthritis); amyloidosis; neoplasms and cytostatic chemotherapy for cancer; steroid use; intravenous drugs. [5]
Pathogenesis
Any abscess should be seen as a tissue defense response to prevent the spread of infection.
Infections implicated in spleen abscess formation include: Gram-positive β-hemolytic group A Streptococcus pyogenes; Staphylococcus aureus; Staphylococcus aureus; Pseudomonas aeruginosa (blue bacillus); Escherichia coli (Escherichia coli); Salmonella (salmonella) of the Enterobacteriaceae family; [6] Enterococcus spp; Klebsiella spp; [7] Proteus spp; Acinetobacter baumannii; Mycobacterium tuberculosis (Mycobacterium tuberculosis); Bacteroides fragilis bacteroides. [8]
Microorganisms use their enzymes to destroy cells and trigger a cascade of oxidative processes, which leads to the secretion and release of proinflammatory cytokines. The cytokine-induced inflammatory reaction leads to an increase in regional blood flow and vascular endothelial permeability, recruitment of large numbers of leukocytes into the infected area and activation of tissue immune cells - mononuclear phagocytes (macrophages).
As a result of the inflammatory process, a purulent exudate is formed, consisting of the liquid part of the blood without formational elements - plasma, active and dead neutrophil granulocytes (destroying bacteria leukocytes-neutrophils), plasma protein fibrinogen and remnants of non-viable cells of the spleen parenchyma that have undergone necrosis.
In this case, the pus is enclosed in a capsule that is formed by adjacent healthy cells to localize the infection and limit its spread as much as possible.
The peculiarity of the pathophysiological mechanism of spleen abscess formation in hematogenous spread of bacterial infection experts consider the initial functions of its red pulp (which makes up about 80% of the parenchyma) - filtration of blood from antigens, microorganisms and defective or spent erythrocytes. In addition, the red pulp of the spleen is a reservoir for white blood cells, platelets, and monocytes. And in the spleen, the population of monocytes (from which macrophages are formed) exceeds their total number in the circulating blood. Therefore, monocytes in the red pulp mobilize very quickly to deal with infection.
Symptoms of the spleen abscess
The first signs of spleen abscess are febrile fever (with body temperature up to +38-39 ° C) and increasing general weakness.
The clinical picture is complemented by pain in the left subcostal and rib-vertebral region (which increases with breathing). When palpating the upper left quadrant of the abdominal cavity, muscle protection (muscle tension) is triggered, and the overlying soft tissues are edematous. [9]
Complications and consequences
Spleen abscess gives complications in the form of: accumulation of air in the pleural cavity (pneumothorax); left-sided pleural effusion; collapse of lung tissue (atelectasis); formation of a subdiaphragmatic abscess or pancreatic fistula; perforation of the stomach or small intestine.
The consequence of spontaneous rupture of the abscess capsule is the entry of purulent exudate into the abdominal cavity with the development of peritonitis.
Diagnostics of the spleen abscess
Diagnosis of splenic abscess is considered a clinical challenge, and instrumental diagnosis - imaging using spleen ultrasound and/or computed tomography, and review chest x-ray - plays a key role. [10]
A spleen abscess on ultrasound usually demonstrates a hypoechogenic area or an anechogenic area (that is, with absent echogenicity) and enlargement of the organ. [11], [12]
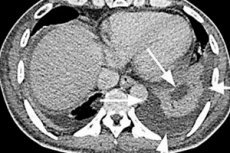
A more reliable method is computed tomography (CT) of the abdominal cavity, the sensitivity of which in the diagnosis of splenic abscess is 94-95%. A spleen abscess on CT looks like a hypodense (low-density) zone, which corresponds to a pus-filled cavity in the organ parenchyma.
General and biochemical blood tests, analysis for inflammatory markers (COE, C-reactive protein), bacteriologic blood culture, Coombs' test (for anti-erythrocytic antibodies in the blood), etc. Are necessary.
The differential diagnosis must take into account the variety of bacterial infection and also distinguish between other conditions that can mimic an abscess: splenic infarction, hematoma, lymphangioma, and splenic lymphogranulomatosis. [13]
What do need to examine?
Who to contact?
Treatment of the spleen abscess
All patients with splenic abscess require hospitalization. Treatment is carried out with high doses of parenteral broad-spectrum antibiotics (Vancomycin, Ceftriaxone, etc.) and transdermal aspiration of pus under ultrasound control (if the abscess is one or two-chambered, with a sufficiently thick wall) or open (abdominal intraperitoneal) drainage of purulent exudate. [14] For more details see. - treatment of abscess with antibiotics
Patients with fungal abscesses are treated with antifungal drugs (Amphotericin B) and glucocorticoids (corticosteroids).
If there is no response to antibiotics with drainage, the method of last choice is surgical treatment - splenectomy (removal of the spleen), which can be performed laparoscopically in many patients. [15]
In addition, therapy should target the underlying cause of the abscess, such as bacterial endocarditis.
Prevention
It is impossible to completely avoid the formation of a spleen abscess, but - to reduce its probability - it is necessary to timely identify and treat all infectious diseases, as well as strengthen the immune system.
Forecast
Undetected and untreated splenic abscess is almost always fatal; the mortality rate is high (more than 70% of cases) and varies depending on the type of abscess and the patient's immune status. But with appropriate treatment, the mortality rate does not exceed 1-1.5%. [16]