Medical expert of the article

New publications
Vocal cord paresis: causes, symptoms, diagnosis
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Speech in human society is the main means of communication, which also contributes to the development of higher mental functions: thinking, attention, memory, etc. From infancy, we learn to understand and reproduce sounds, words, phrases. These generally accepted signals and their configurations facilitate mutual understanding between people. Modern man does not even think about how to express his thoughts, attitudes, emotions in other ways so that they are understandable to others and help build relationships. It is not surprising that any pathologies of the vocal apparatus (for example, paresis of the vocal cords), depriving a person of the ability to normal verbal (speech) communication, are a serious problem today, and not only of a medical nature.
A little bit of anatomy
It is no secret that speech is an important feature of humans, which distinguishes them from other representatives of the animal world. Their speech apparatus is a complex structure, which includes organs related to various functional systems. The speech apparatus consists of 2 sections: central and peripheral. The peripheral section includes:
- the auditory apparatus (outer, middle and inner ear), which enables us to hear sounds and speech,
- speech apparatus (respiratory, vocal and articulatory apparatus) with the help of which we can produce different sounds, form various sound combinations and words.
The central section of the speech apparatus includes the speech zones of the brain and nerve fibers that transmit impulses from the central nervous system to the peripheral organs of respiration and speech involved in sound production, and in the opposite direction. This gives us the ability not only to pronounce individual sounds, but also to control their pronunciation, analyze and form certain chains of sounds (words) that we use to denote a particular object, action, characteristic, etc. [ 1 ]
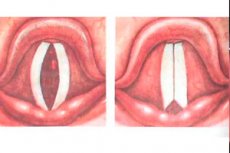
The basis of the vocal apparatus is the larynx, which consists of cartilage and muscles and is covered with a mucous membrane. In the upper part of the larynx, which is basically the sound generator, its inner membrane forms 2 folds consisting of muscular and fibrous connective tissue. The connective tissue parts of the folds are called vocal cords, although most often this term refers to the vocal folds, i.e. their muscular and connective tissue parts.
Due to movements in the joints of the larynx, the presence of elastic muscles and nerve fibers innervating them, the tissue of the vocal folds can contract and stretch. As a result, the tension of the vocal cords and the size of the gap between them change, under the influence of the stream of exhaled air, vibration of the cords occurs (both their entire mass and individual parts) and a sound of different tonalities is formed.
The vocal cords change their position and tension under the influence of nerve impulses coming from the central part of the speech apparatus. The impulses go along the nerve fibers. It is clear that any damage to the nerves connecting the central nervous system and the vocal apparatus will certainly affect the quality of pronunciation.
Epidemiology
And although, according to statistics, people whose profession requires them to speak a lot most often seek help for a lost or hoarse voice: teachers, dispatchers, announcers, etc., it is important to understand that a heavy load on the vocal cords is far from the only reason for the disruption of voice formation. Moreover, in this case we are talking about a simple reversible type of paresis associated with a disruption of blood supply (due to overstrain of the cords, small capillaries can burst, nutrition of nearby soft tissues deteriorates, the tone of the muscles of the larynx and vocal folds decreases).
According to research, 60% of vocal cord paresis are associated with neoplasms in the larynx, esophagus or thyroid gland and surgical operations in the same localization. Moreover, thyroid surgery comes first. Idiopathic paresis of uncertain etiology is diagnosed in 20% of cases, and usually the real cause of the disease is a viral infection. Paresis due to nerve damage during neurosurgical operations and neurological pathologies occurs in 5% of cases. Infectious and inflammatory diseases of the brain, throat, and respiratory system cause dysfunction of the vocal apparatus in 4-5%. [ 2 ], [ 3 ], [ 4 ]
Benninger et al. calculated that bilateral vocal cord paralysis could be associated with surgical trauma in 44% of cases, malignancy in 17% of cases, secondary to tracheal intubation in 15% of cases, neurologic disease in 12% of patients, and idiopathic causes in 12% of cases.[ 5 ]
Thus, it becomes clear that vocal cord paresis is a multifactorial pathology that requires careful examination and identification of the causes of the disease. Only in this way can the doctor understand the mechanism of the resulting phonation (sound production) disorder and prescribe appropriate treatment (symptomatic and aimed at eradicating the cause of the disease).
Causes vocal cord paresis
Paresis is a partial loss of vocal apparatus functions, which can be considered as an independent disease or occur against the background of other pathologies. Most often, such a violation of phonation is observed against the background of inflammatory diseases of the larynx:
- Laryngitis is an inflammation of the larynx due to the negative impact of infection, irritation of the laryngeal mucosa by inhaled chemicals or acids entering the oral cavity (from there they can also enter the initial sections of the larynx) with reflux disease, overstrain of the vocal folds during loud talking, shouting, during vocal exercises. Causes can also be traumatic injuries, the spread of the inflammatory process from the lower or upper respiratory tract to the laryngeal mucosa, tumors in the neck and mediastinum, age-related decrease in muscle tone, as a result of which food enters the respiratory tract and can provoke inflammation. [ 6 ]
- Laryngotracheitis is an inflammation of the mucous membrane of the larynx and the initial sections of the adjacent trachea. It is usually of infectious origin (usually viral, less often bacterial) and occurs as a complication of infectious and inflammatory diseases of the nose, throat, bronchi, and lungs. Although the allergic nature of the disease cannot be ruled out.
Inflammation is always accompanied by metabolic disorders (tissue edema), hyperemia (reddening of the mucous membrane due to circulatory disorders) and, as a result, decreased muscle tone of the larynx. It is not surprising that with the above-described pathologies, coarsening or hoarseness of the voice, a decrease in its strength are noted, and if you do not take care during the illness, then a complete lack of voice or whispered speech. [ 7 ]
- Chondroperichondritis of the laryngeal cartilages with paresis of the vocal cords is an inflammatory disease of the cartilaginous tissue of the main organ of phonation. The cricoid and arytenoid cartilages, to which the vocal cords are attached, are most susceptible to the disease. [ 8 ] Voice changes in this case are observed in parallel with a violation of the act of swallowing. The cause of the disease is called an infection. These can be opportunistic and pathogenic bacteria, viruses that penetrate and become active in the tissues of the larynx as a result of stab and gunshot wounds, burns, respiratory diseases, internal infections (tuberculosis, syphilis, pneumonia, typhus), erysipelas. Sometimes chondroperichondritis of the larynx develops after blunt trauma to the throat, as a complication after surgical interventions and medical manipulations (intubation, bronchoscopy, tracheotomy, esophageal bougienage, etc.). [ 9 ] In some cases, the disease was provoked by radiation therapy for cancer, which reduced the body's resistance to infection. [ 10 ] If the disease is neglected, the voice may not recover on its own.
Risk factors
Risk factors for such a complication as vocal cord paresis can be considered any respiratory infectious disease (ARI, flu, tonsillitis, bronchitis, inflammation and tuberculosis of the lungs, diphtheria), as well as infections of the brain (meningitis, meningoencephalitis) and spinal cord (poliomyelitis).
Sound production disorders can be diagnosed in certain infectious pathologies of the gastrointestinal tract (for example, when the respiratory tract is affected by the typhoid fever pathogen, the voice changes, it becomes hoarse, muffled; with botulism, a nasal voice is often observed), typhus, serious head injuries, the formation of local voids in the spinal cord and brain (syringobulbia), syphilitic infection, cerebral palsy.
In neuromuscular autoimmune pathology called "myasthenia", vocal cord paresis can occur as a result of strong tension in the larynx muscles (long or loud conversation, eating, etc.). In severe poliomyositis (inflammatory lesion of striated muscles), the soft tissues of the neck and larynx can become inflamed, which is accompanied by a partial disruption of their functionality (weakening, decreased tone).
Dysfunction of the vocal cord muscles may be associated with vascular disorders of the brain (cerebral atherosclerosis, cerebral stroke), tumor processes in it (near the speech centers and the passage of nerves responsible for the innervation of the larynx) and neurosurgical operations (for example, with partial damage to the nuclei of the vagus nerve). Paresis of the vocal cords after surgery caused by damage to the vagus nerve (its nuclei and branches) is a rare complication observed in 5-6 patients out of 100.
One of the most common causes of vocal cord paresis is considered to be tumor processes in the neck and mediastinum, which compress the nerves that conduct impulses to the peripheral part of the speech apparatus, and laryngeal trauma, when the vagus nerve or its branches are damaged: the recurrent and inferior laryngeal nerve. Most often, we are talking about damage to the recurrent laryngeal nerve, which is possible during surgical interventions on the thyroid gland, intubation, brachial plexus block using the ladder method, external trauma to the larynx. [ 11 ]
Compression and dystrophy of the recurrent nerve is possible with various diseases of the chest organs. The branches of the vagus nerve, going in the opposite direction (from the chest organs to the pharynx and larynx), directly contact many vital organs (heart, lungs, esophagus, mediastinum, thyroid gland). Any pathological formations and processes in the tissues of these organs can:
- put pressure on a nerve (aortic aneurysm, inflammation of the membranes or enlargement of the lower chambers of the heart, tumors, goiter, pneumonia with their enlargement, exudative and cicatricial processes in the pleura)
- or cause its destruction (oncological diseases: esophageal cancer, malignant processes in the thyroid gland, mediastinum, etc.).
The recurrent nerve can also be compressed by enlarged lymph nodes (cervical, peribronchial, mediastinal). [ 12 ]
Increased strain on the vocal cords and inhalation of cold air through the mouth provoke inflammatory diseases of the tissues of the pharynx and larynx, which disrupt their blood supply and functionality. An identical situation is observed when inhaling heavily dusty air, smoke, caustic chemicals, as well as with severe intoxication of the body. In this case, laryngitis is diagnosed, which has a complication in the form of paresis of the vocal cords.
Since the peripheral part of the speech apparatus is directly connected with the activity of the central nervous system, any disturbances in its work can negatively affect the process of sound formation. Paresis of the vocal cords can be observed in psychopathy, hysterical attacks, neuroses (for example, astheno-neurotic syndrome), neurocirculatory dystonia (aka vegetative-vascular or VSD). Sometimes people's voice disappears or weakens greatly due to nervousness as a result of stress or severe psycho-emotional shock. [ 13 ]
Another extremely rare cause of bilateral recurrent laryngeal nerve palsy is Guillain-Barré syndrome (GBS), the most common acquired demyelinating neuropathy. Although Guillain-Barré syndrome classically presents as loss of deep tendon reflexes with ascending muscle paralysis, cranial nerves may be affected in addition to peripheral nerves. GBS may also present with respiratory distress syndrome requiring mechanical ventilation, development of cardiac arrhythmias, and hemodynamic instability.[ 14 ]
Pathogenesis
The pathogenesis of the disease called vocal cord paresis is based on a disruption of nerve conduction (the vagus nerve and its branches), which transmit impulses to the tissues of the larynx, including the muscle tissue of the vocal folds. That is, we are talking about a disruption of the innervation of the vocal apparatus, which is the cause of a decrease in the tone of its muscles and is reflected in the strength, sonority, and timbre of the voice. These disorders in speech therapy are combined under one name - dysphonia, and in the case of a complete absence of voice, they speak of aphonia. [ 15 ], [ 16 ]
Vocal cord paresis and its consequences have no gender or age preference. This pathology can occur with equal probability in men, women, and children. [ 17 ]
Symptoms vocal cord paresis
Considering the fact that vocal cord paresis is a multifactorial disorder of the speech apparatus functionality, one can suspect that the combinations of symptoms in different types of pathology may differ significantly. In fact, if we discard the symptoms of the underlying disease (and weakening of the muscular-ligamentous apparatus of the larynx is often observed against the background of existing health problems), a specific clinical picture is visible in all cases.
The first signs of vocal cord paresis are usually changes in the voice (its sonority, timbre, tone) and breathing problems. These symptoms can be expressed to varying degrees. In case of unilateral cord paresis, unpleasant changes in the voice come to the fore. It becomes unusual, more hoarse, muffled, husky. Often, a coarsening of the voice and an unusual rattling of sounds during a conversation are noted.
Rapid fatigue when you have to talk a lot, associated with tension when exhaling (the sound is formed when exhaling), is explained by the same changes in the voice. The formation of sounds and words in humans is carried out at a reflex level. Having learned to speak, we no longer think about how to reproduce this or that sound. But with paresis, sounds change, their sound becomes unusual, so a person has to strain the vocal apparatus more to return the sonority of the voice and correctly pronounce sounds and words. This leads to rapid fatigue, discomfort in the larynx, and sometimes to a spasm of its muscles.
Breathing problems with vocal cord paresis are explained by the narrowing of the glottis as a result of decreased muscle tone of the folds. The fact is that the trachea is not only an organ of phonation, but also part of the respiratory system. When we are silent, they are open, and air can freely circulate in the respiratory tract. The vocal folds close only during conversation. If their tone is reduced as a result of weakening central control or tissue trophism, the folds remain closed or do not fully open even during silence, which is an obstacle to air flow.
In case of unilateral paresis of the vocal cords, which occurs when their innervation is disrupted on one side, there are no particular breathing problems. A normally functioning vocal fold allows a gap to form that is sufficient for the free passage of air and pronunciation, even if somewhat distorted. After several months, pronunciation defects become less noticeable, since the lost function of the affected fold is compensated for by the normal functioning of the healthy one, which now works for two.
But when it comes to bilateral paresis, the situation is somewhat different. Narrowing of the glottis on both sides is already a serious problem for breathing, inhalation and exhalation are difficult for a person. This is especially noticeable during physical exertion, when shortness of breath occurs, or during a lively conversation (a person speaks with aspiration, makes frequent pauses to take a breath, inhalation and exhalation are unusually noisy).
In addition, with weak vocal cords, it becomes impossible to pronounce most, and sometimes even all, speech sounds. In such a case, the patient either speaks in a whisper or communicates with gestures (aphonia). However, a complete lack of phonation with paresis is extremely rare, unlike with paralysis of the vocal cords, when the ability to produce sounds and breathe completely depends on the position that the affected cords maintain. Thus, bilateral paralysis with closed cords can lead to sudden asphyxia and death of the patient.
Despite the fact that the larynx is not an organ of the digestive system, many patients with paresis of the vocal cords, which are located in close proximity to the pharynx, have difficulty swallowing food. If the weakening of the functionality of the vocal cords is combined with a violation of the innervation of the epiglottis, which blocks the entrance to the larynx during eating, the risk of food entering the respiratory tract increases: the larynx and trachea, which can also cause asphyxia.
Unilateral vocal cord paresis may be accompanied by decreased functionality of other nearby organs (tongue, lips) and dysphagia (swallowing disorder) as a result of damage to the nerves responsible for innervation of various organs of the head and neck. Thus, the vagus nerve (or rather a pair of nerves) conducts impulses from the brain to the abdominal cavity, and its branches are responsible for innervation of not only the articulatory apparatus, but also other areas of the head, neck, chest, and abdominal cavity. This nerve contains both motor and sensory fibers, so its damage may be accompanied by both a violation of the motor function of organs and a decrease in their sensitivity (numbness).
When the vagus nerve and its branches are damaged, the central nervous system partially or completely loses control over the functioning of a particular part of the body (in particular, the larynx and oral cavity organs), so conscious volitional efforts do not allow for the process of sound production to be corrected in a short time.
In functional paresis that occurs in people with an unstable psycho-emotional state, the clinical picture may differ somewhat. It includes non-specific symptoms that are often subjective. In the vast majority of cases, such symptoms are expressed much weaker than patients describe them. Patients may complain of a sore throat, tickling or burning sensation in the throat, a lump in the throat, etc., as well as headaches, sleep disorders, increased anxiety, which are not directly characteristic of paresis.
Forms
The variety of causes of vocal cord paresis has necessitated the classification of paresis depending on the factors that cause it. Thus, disorders of sound production (dysphonia) are usually divided into organic and functional. Organic disorders include cases of dysfunction of the vocal apparatus caused by inflammatory diseases, neoplasms in the vocal folds, and motor disorders (paresis and paralysis of the muscles of the larynx and vocal cords in particular).
If there are no signs of inflammation, the shape and color of the vocal cords are normal, but there is vocal dysfunction, otolaryngologists talk about functional dysphonia caused by an incorrect relationship between the processes of excitation and inhibition in the brain or functional psychogenic disorders.
Previously, it was customary to divide paresis of the vocal cords and larynx into 2 types:
- myogenic (myopathic)
- neurogenic (neuropathic).
Myogenic changes were those in the inner layers of the muscular tissue of the larynx, caused by acute and chronic inflammation, vocal apparatus strain, intoxication, etc., i.e., disturbances in the blood supply and nutrition of the muscles. Neuropathic paresis was considered to be paresis caused by weakness of the muscles of the vocal cords due to a disturbance in their innervation (compression, damage, nerve dysfunction). [ 18 ]
Today, some scientists classify myopathic paresis of the vocal cords as functional dysphonia of the hypotonic type and consider it as a temporary phonation disorder that is restored by local action on the muscles. And only those pathological conditions that are associated with a disorder of the vagus nerve and its branches, i.e. neurogenic pathologies, are considered laryngeal paresis.
Neuropathic forms of paresis can be both organic and functional, i.e. arising due to neuropsychiatric disorders. Organic disorders are divided into pathologies of central and peripheral origin.
Paresis of central origin, the causes of which are diseases of the brain and operations on it, make up only 10% of the total number. These include: damage to the cortex of the cerebral hemispheres, corticonuclear pathways (bundles of nerve fibers that transmit impulses to the motor nuclei of the cranial nerves, in this case we are talking mainly about the fibers going to the nerve centers of the vagus nerve) or directly to the nuclei of this nerve located in the medulla oblongata. They occur as a result of cerebral ischemia, tumors in it, serious head injuries, infectious and inflammatory processes in the brain and spinal cord. Functional weakness of the vocal cords can be diagnosed in cerebral palsy, multiple sclerosis or be the result of errors during neurosurgical interventions.
Paresis of peripheral origin occurs as a result of damage to the nerves that transmit information from the brain to the ligaments and back. Such nerves are precisely the branches of the vagus nerve. Causes: nerve injuries, its compression by various neoplasms and enlarged organs of the chest, lymph nodes, metastasis of cancerous tumors, etc.
A distinction is also made between congenital and acquired paresis. In the first case, the pathology is provoked by a disruption in the formation of various parts of the speech apparatus during the prenatal period (infections, intoxications, vitamin deficiency in the pregnant woman in the early stages, fetal trauma) or birth injuries that lead to a disruption in the innervation of the peripheral part of the speech apparatus in the infant. Acquired weakness of the vocal apparatus is a consequence or complication of other pathological processes or the result of overstraining the vocal apparatus, although in most cases we are talking about the impact of several provoking factors at the same time, for example, active conversation and inhalation of cold air, overstrain of the muscles of the vocal cords against the background of an existing disorder of the central nervous system, etc.
Vocal cord paresis can be either unilateral (considered the most common and characterized by damage to the right or left vocal cord) or bilateral, [ 19 ] when both vocal cords are affected. Despite the variety of causes and factors that can cause paresis of the left or right vocal cord, [ 20 ] unilateral pathology is considered less dangerous, since it mainly concerns phonation disorders and associated psychological problems.
In case of bilateral weakening of the ligaments, developing as a complication after operations on the neck and thyroid gland, against the background of injuries, intubation, neurodystrophic and neuromuscular diseases, we are talking not only about a simple violation of sound formation, but also about a pathology of the respiratory function, which is considered a life-threatening situation.
Complications and consequences
Human speech is the ability to fully and thoroughly communicate with other representatives of one's species, the ability to convey one's thoughts in an understandable form and to receive useful information from other people. People with phonation disorders (due to various reasons) do not experience a decrease in understanding of other people's speech, but the inability to express one's thoughts clearly and understandably definitely becomes a serious psychological problem. This is especially noticeable if a person's professional activity places demands on pronunciation.
A teacher with a hoarse voice finds it difficult to speak and hold the attention of students, which entails a violation of discipline and the assimilation of the material presented. A speech therapist without clear pronunciation of sounds cannot teach his charges to speak correctly. A singer with dysphonia does not have the right to start working at all, which is accompanied by a certain discontent on the part of the management and sponsors. Thus, paresis of the vocal cords and the resulting violation of the voice function not only limits the possibilities of normal communication, but can also cause a person's disability, especially in the case of dysfunction of the nerves associated with their damage (dystrophic processes, careless resection), which are often irreversible.
Dysphonia does not have the best effect on children, especially if such a disorder arose at an early age, when the child is just learning to speak. The sooner the problem is solved, the fewer consequences it will have. After all, the developed incorrect stereotypes of pronunciation of sounds will subsequently be very difficult to change, despite the restored voice function. This will create difficulties in communication, and in understanding words, in comprehending educational material. [ 21 ]
It is especially hard for people who lose their voice completely. They become virtually mute while retaining their hearing and understanding of speech. This condition is psychologically difficult for most patients: they withdraw, try to limit contacts, and become depressed.
Paresis caused by infectious and inflammatory diseases or neuropsychiatric disorders is usually reversible, and with appropriate treatment the voice is quickly restored. However, patients do not always seek special help, expecting the disease to go away on its own, and they start the pathology. But the longer the vocal cords experience a lack of oxygen and nutrients, the harder it will be for them to recover from the disease. [ 22 ]
Full treatment of neuropsychiatric disorders is impossible without the participation of specialists (psychologist, psychiatrist), and without stabilization of the central nervous system, the return of the voice can take a very long time.
Diagnostics vocal cord paresis
Vocal cord paresis is a pathology that can have completely different, unrelated causes. Its external manifestations in the form of dysphonia (aphonia) can say little about the factors that led to the disruption of voice production. And it is too early to make a diagnosis based only on this, because weakness of the vocal cord muscles does not occur by itself. It should be considered as a complication of existing pathologies and functional changes in the work of organs caused by metabolic disorders, infection, intoxication, nerve damage during surgery, etc.
That is, dysphonia, which is precisely the main symptom of cord paresis, is considered an independent disease only in isolated cases. For example, with weakness of the vocal folds in newborns. But even in this case, it is rather a remote consequence of intrauterine disorders that led to such anomalies in the child's development.
In most cases, patients seek medical attention not so much because of dysphonia itself (unless it is a pronounced form or the voice is used by a person as a working instrument), but because of breathing and swallowing disorders, suspecting cardiopulmonary diseases, diphtheria, tonsillitis, croup (in a child), etc. In some cases, vocal cord paresis is diagnosed unexpectedly, in parallel with the underlying disease, about which it is necessary to consult a doctor (this often happens with respiratory diseases, endocrine pathologies, tumor processes, heart diseases, esophagus, etc.).
Be that as it may, but the diagnosis of voice formation disorder and identification of the causes of this process begins with a visit to the doctor. First, patients contact a therapist who decides whether he can make a diagnosis on his own (for example, with dysphonia due to infectious and inflammatory diseases of the throat and respiratory system) or whether the help of narrow specialists will be required: an otolaryngologist, neurologist, neurosurgeon, psychiatrist, pulmonologist, endocrinologist, etc. If we are talking about dysphonia against the background of overstrain of the muscles of the vocal apparatus, a consultation and help of a phoniatrist may be needed, to whom people who are professionally engaged in vocals usually turn.
When visiting a doctor for the first time, specialists rely on the patient's complaints, visual examination of the throat, and anamnesis. Information about past and existing illnesses, surgical interventions performed allows one to quickly get their bearings in the situation and narrow the range of possible causes of dysphonia, respiratory failure, and dysphagia, which are manifestations of vocal cord paresis. Thus, a tendency to psychogenic pathologies allows one to assume functional paresis, and operations on the chest, mediastinum, heart, thyroid gland, esophagus, as well as neurosurgical interventions can be considered as a possible cause of organic damage to the vagus or recurrent nerve.
But this information is not enough. Laboratory tests also cannot reveal a clear picture of the pathology. With their help (blood test) it is only possible to determine the presence of inflammatory processes in the body and some metabolic disorders (for example, elevated glucose levels in diabetes).
Special tests prescribed when malignant diseases are suspected (biopsy and histological examination of the biopsy) only provide the opportunity to differentiate a malignant tumor from a benign one, but are not an indicator that it is the neoplasm that has caused the disruption of the functionality of the vocal cords and pronunciation.
Instrumental diagnostics play a decisive role in the diagnosis of vocal cord and laryngeal paresis. The simplest and most accessible method used by otolaryngologists is laryngoscopy – examination of the throat and larynx using instruments. Indirect laryngoscopy uses a mirror and a headlamp for illumination. Direct laryngoscopy is performed using a laryngoscope inserted into the patient’s larynx (both a diagnostic and therapeutic procedure), which allows visualization of both the vocal folds and the inner part of the larynx. [ 23 ]
Laryngoscopy allows to detect inflammatory foci, changes in the mucous membrane of the larynx, small and large hemorrhages that are not noticeable during a normal examination. It can be used to assess the condition of the vocal folds: their position during breathing and phonation, pathological changes in movement, color, shape, size of the glottis.
An electronic stroboscope is used to determine the nature of vocal cord vibrations. It allows one to evaluate the presence or absence of vocal cord vibrations during sound reproduction, the uniformity and synchronicity of existing vibrations in frequency and amplitude, to identify incomplete closure of the cords, the shape of the glottis, etc.
For greater objectivity of the study, videolaryngoscopy or videolaryngostroboscopic examination may be prescribed, which allows an enlarged image of the larynx to be displayed on the monitor, recorded, and information documented for subsequent discussion among specialists.
A relatively new method for studying the phonation characteristics of the voice is glottography. A glottograph is a device that generates ultra-high frequency currents and measures the resistance when these currents pass through the larynx. The functionality of the vocal folds can be judged by the change in current strength. On the device monitor, you can see a curve that in healthy people is characterized by pronounced cyclicity and uniformity of individual cycles. In various pathologies, the curve has certain deviations: the periodicity is disrupted, the oscillation phases are not determined, specific fragments with teeth appear. [ 24 ]
If the doctor detects a failure of the vocal folds to close, limited mobility of one of them (or both), or other abnormalities that allow one to suspect a failure of muscle tissue or insufficient nervous regulation, the patient is referred for additional examination. Methods are used to help assess the contractility of the laryngeal muscles (electromyography) and the characteristics of neuromuscular transmission (electroneurography). However, electromyography does not provide sufficient information about the oscillations of the vocal folds and is indicative of laryngeal paresis, which can be combined with weakening of the vocal cords, and neurography is relevant only in the case of a neurogenic nature of the pathology and is prescribed after consultation with a neurologist. [ 25 ]
If central genesis paresis is suspected (bulbar, associated with pathologies of the medulla oblongata, where the nucleus of the vagus nerve is located, or cortical, associated with damage to the cerebral cortex and its conducting pathways), a thorough examination of brain structures for the presence of tumors, hemorrhages, and degenerative processes is required. Such a study is possible using computed tomography or magnetic resonance imaging of the brain, as well as scanning of brain structures (MSCT), carried out in cases of trauma, to identify developmental anomalies, acute hemorrhages. [ 26 ], [ 27 ], [ 28 ]
If the doctor suspects peripheral paresis of the vocal cords, i.e. the one caused by compression of the branches of the vagus nerve on its way to the vocal apparatus, a general chest X-ray, tomography of the mediastinum or esophagus, ultrasound diagnostics of the heart and thyroid gland are prescribed.
Radiography and tomography of the larynx help to assess the overall picture of the organ, but do not provide the ability to determine the nature of the movements of the vocal folds, so such studies are more relevant for identifying tumors and degenerative processes in the tissues of the larynx or near it. [ 29 ], [ 30 ]
If the patient's examination does not show any morphological changes (the structure and shape of the vocal cords are normal, no organic disorders that could affect the function of sound production were found in the body), the doctor concludes that the paresis may be functional. In this case, it would not be superfluous to consult a psychologist and psychiatrist, conduct psychological testing with diagnostics of possible psycho-emotional disorders.
Differential diagnosis
Particular attention is paid to differential diagnostics, because it is much easier to diagnose paresis or paralysis of the vocal cords than to determine its cause. Deafening and hoarseness of the voice can be observed both in respiratory pathologies, which is a common situation and does not require specific treatment (often standard procedures for treating a sore throat are sufficient), and in neurological disorders, which can only be identified with the help of special instrumental studies. Therefore, when establishing the true cause and picture of the pathology, a large role is played by the community of doctors of various fields.
Vocal cord paresis must be distinguished from their paralysis. In the first case, we are talking about incomplete loss of functions of the nerves that innervate the vocal folds, i.e. about weakening of their functionality. In case of vocal cord paralysis, innervation is absent, which is visible during microlaginoscopy (displacement of the laryngeal mucosa due to low tone of the vocal fold muscles) and electroglottography.
The need to differentiate myopathic and neurogenic pathology is associated with different approaches to the treatment of diseases of various etiologies. And in some cases, we are talking about a violation of the innervation of not so much the vocal cords, but the articulatory apparatus. The causes of the pathology may be the same (damage or compression of the nerves), but in addition to the vagus nerve, in this case, the pathology of the glossopharyngeal and hypoglossal nerves (their peripheral parts and nuclei located in the medulla oblongata) is considered. Here, there is also an incorrect pronunciation of individual sounds, a change in the strength and timbre of the voice.
Who to contact?
Prevention
The diagnosis of "vocal cord paresis" sounds somewhat menacing, so one might get the impression that we are talking about a severe, irreversible pathology of the speech apparatus. In fact, the prognosis of the disease and the approach to its treatment depend on the severity of the disorder.
Myopathic paresis, developing as a complication of laryngitis and other infectious and inflammatory diseases of the respiratory tract or as a result of excessive strain on the vocal cords, is quite easily treated with simple methods and passes without consequences. Functional disorders of the vocal apparatus, arising against the background of stress and nervous disorders, are also not considered irreversible. The speech function is restored as the psycho-emotional state stabilizes (in some cases it even passes without treatment).
In most cases of neurogenic paresis, the patient manages to restore his voice and correct pronunciation, but there is no longer any talk of restoring vocal abilities. Moreover, some patients continue to have pronunciation defects, and some difficulties in controlling their vocal apparatus are determined. In the case of severe organic disorders that are difficult to treat, a decrease in vocal function is observed for a long time, which leads to atrophy of the muscles of the vocal cords and persistent phonation disorders. [ 31 ]
Prevention of vocal fold dysfunctions consists of taking good care of your voice, preventing and promptly treating infectious and inflammatory diseases of the throat and respiratory tract, and maintaining your nervous and endocrine systems in good condition.
In childhood, dysphonia usually occurs against the background of laryngitis, so parents should pay close attention to ensuring that the child does not overheat before going outside, does not drink ice water, does not try to use icicles as ice cream, talks less in the cold, etc. From a young age, it is necessary to explain to children in an understandable form what such carelessness can end up with, because only awareness of the dangerous consequences of their actions works better than simple lectures and punishments.
Adults are often careless about the air we breathe. Working in dusty conditions, at chemical plants, in laboratories, workshops, they do not always adhere to the requirements for protecting the respiratory system. But irritants can easily affect the functionality of both the respiratory and vocal apparatus, which will change the nature of speech and its capabilities. The requirement to wear respirators, cotton-gauze bandages and other protective equipment is due to the need to protect the respiratory system and voice formation, which are vital for humans. This is the prevention of many diseases, including paresis of the larynx and vocal cords, which is characterized by dysphonia or aphonia.
People of certain professions, especially teachers, whose voice is a decisive factor in the education and upbringing of the younger generation, with all the desire, are not always able to maintain the health of the vocal cords. In this case, the emphasis will have to be on the prevention of complications of paresis of the vocal cords, i.e. dystrophic processes as a result of long-term dysfunction of the vocal apparatus. It is better to take care and talk less during the acute period of the disease, which will help the cords to recover faster. Otherwise, you can wait a long time for the voice to recover, and you also need to be prepared that it will subsequently have some unpleasant features.
Early diagnostics of the pathology called "vocal cord paresis" is the key to effective treatment of the vocal apparatus (as well as other systems associated with it) and voice restoration. Therefore, you should contact a doctor at the first signs of phonation disorders: changes in the timbre and sonority of the voice, its strength, rhythm, especially if they occur in the postoperative period or against the background of organic diseases of the brain. But myopathic paresis should not be treated carelessly either, because dysfunction of the vocal apparatus over a long period of time, impaired breathing and nutrition of the tissues of the vocal apparatus in inflammatory diseases can provoke the development of degenerative processes that affect the quality of the voice, the communicative function and the life of the patient in general.