Medical expert of the article

New publications
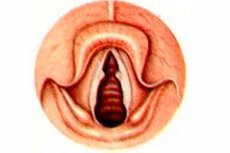
Vocal fold nodules
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Professional diseases of the vocal apparatus (chronic laryngitis; vocal fold nodules) are diseases of the larynx that develop in people with voice-speech professions when performing professional voice functions or during prolonged (without rest) vocal activity, as a result of inept use of phonation breathing, modulation of pitch and volume of sound, incorrect articulation, etc.
Vocal fold nodules, also called "singer's nodules" or hyperplastic nodules, are small paired nodules, symmetrically located on the edges of the vocal folds on the border of their lateral and middle thirds, of very small size (pinhead), consisting of fibrous tissue. Sometimes they take a diffuse form and spread over a large surface of the folds, causing significant disturbances in the timbre of the voice.
Epidemiology
The prevalence of occupational diseases of the pharynx and larynx among people in voice and speech professions is high and reaches 34% in some professional groups (teachers, educators). Moreover, a clear dependence on length of service is noted, the incidence is higher in groups examined with more than 10 years of experience.
Causes vocal fold nodules
Professional diseases of the vocal apparatus develop in teachers, kindergarten teachers, vocalists, dramatic actors, announcers, tour guides, etc. Of particular importance in this case is work in a foreign language, when errors in speech technique cause a sharp tension of the neck muscles, and insufficiently good respiratory support leads to a significant displacement of the larynx forward, which reduces the tone of the vocal folds.
In addition to the main etiological factor (vocal apparatus overstrain), the specifics of working conditions (neuro-emotional stress, increased intensity of ambient background noise, poor room acoustics, changes in ambient temperature, increased dryness and dustiness of the air, uncomfortable working posture, etc.) are important in the development of occupational diseases of the vocal apparatus. Poor vocal hygiene (smoking, alcohol) and inflammatory diseases of the nasal cavity and pharynx contribute to the development of occupational diseases of the larynx. Allergization of the body with the development of increased sensitivity to such irritants as dust, paint spills from scenery, make-up, as well as fatigue and psychogenic trauma play a significant role.
It is also suggested that the etiological factor of vocal fold nodules may be submucous microhematomas, which form under extremely strong vocal load, after the resorption of which fibrous proliferation of connective tissue occurs with the formation of nodules. However, this assumption is rejected by Ch. Jackson (1958), who believes that vocal fold hematomas underlie the formation of polyps.
 [ 6 ]
[ 6 ]
Pathogenesis
These nodules are not tumors in the morphological sense of the term, but look like growths of the vocal fold's own connective tissue. These formations usually occur when they are overstrained during shouting, singing, reciting in a loud voice, especially, according to a number of foreign phoniatric studies, in cases where high-register sounds are used in voice production, which is why vocal nodules are found in sopranos, coloratura sopranos, tenors and countertenors, and very rarely in contraltos, baritones and basses.
Stroboscopic studies have shown that at the level where vocal nodules arise, during high-pitched phonation, the vocal folds take on a more convex shape and thus adhere to each other more closely and for a longer period of time. As a result, a bilateral limited inflammation focus first arises at the indicated location, followed by hyperplasia of the connective tissue fibers, which are most sensitive to mechanical and inflammatory stimuli, during continued vocal loads.
Vocal fold nodules can sometimes develop into “polyps” that have the same histological structure as the nodules that preceded them, and therefore the same pathomorphogenesis.
Symptoms vocal fold nodules
The main complaints of people using the vocal apparatus in their professional activities are rapid vocal fatigue, the sound of the voice in an incomplete range (the voice "sits down"), a feeling of discomfort in the throat, dryness, and irritation. Among workers with experience in the profession from 3 to 10 years, voice disorders (dysphonia) up to complete hoarseness (aphonia), pain in the throat and in the neck area when performing voice-speech functions are noted.
The initial period of the disease is characterized by the development of functional disorders in the vocal apparatus, most often manifested in the form of phonasthenia. Phonasthenia (from the Greek phone - sound and asteneia - weakness) is the most typical functional disorder, which occurs mainly in people of voice and speech professions with an unstable nervous system. The main reason for its occurrence is an increased vocal load in combination with various unfavorable situations that cause disorders of the nervous system. Patients with phonasthenia are characterized by complaints of rapid fatigue of the voice; paresthesia in the neck and throat; soreness, irritation, tickling, burning; a feeling of heaviness, tension, pain, spasm in the throat, dryness or, conversely, increased mucus production. Quite typical for this pathology are the abundance of complaints and their careful detailing by the patient. In the initial stage of the disease, the voice usually sounds normal, and endoscopic examination of the larynx does not reveal any deviations from the norm.
Often, the development of vocal fold nodules is preceded by catarrhal laryngitis and long-term phonasthenia. The latter forces the patient to strain the vocal apparatus, and the former promotes proliferative processes, which can result not only in nodules, but also in other benign tumors of the larynx. In the initial period of nodule formation, patients feel slight fatigue of the vocal apparatus and inadequate formation of singing sounds when playing piano (quiet sounds), especially in high tones. Then, the voice becomes deformed with any sounds: a feeling of a "split" voice, an admixture of vibratory sounds is created, while loud speech requires significant strain of the vocal apparatus. This is due to the fact that during phonation, the nodules prevent the vocal folds from closing completely, due to which the resulting gap causes increased air consumption, the subglottic air support decreases, and the voice strength cannot reach the desired level. Changes are detected during laryngoscopy.
In children, vocal fold nodules are most often observed at the age of 6-12 years, more often in boys, whose vocal apparatus in the stage of hormonal development is more susceptible to alteration during vocal loads. It should be borne in mind that children's games at this age are invariably accompanied by corresponding cries. It has been noted that the formation of vocal fold nodules in children is often accompanied by secondary catarrhal laryngitis caused by the presence of adenoids and impaired nasal breathing. Removal of adenoids in such children, as a rule, leads to the spontaneous disappearance of vocal fold nodules.
Forms
Diagnostics vocal fold nodules
Diagnosis of vocal fold nodules is usually straightforward. The main distinguishing feature is the symmetry of the nodules, the absence of other pathological endolaryngeal signs, and anamnesis data. Sometimes, a young laryngologist inexperienced in laryngeal pathology may mistake vocal processes of the arytenoid cartilages for vocal nodules, which, due to an individual feature, protrude into the glottis, but during phonation, their functional purpose and their absence between the vocal folds, which completely close, become obvious. To verify this, it is sufficient to conduct a stroboscopic examination of the larynx.
The diagnosis of phonasthenia requires the mandatory use of modern methods for studying the functional state of the larynx - laryngostroboscopy and microlaryngostroboscopy. Characteristic findings in laryngostroboscopy in these patients are an unstable and "variegated" stroboscopic picture, asynchronism of vocal fold vibrations, their small amplitude, frequent or moderate tempo. Typical is the absence of "stroboscopic comfort", that is, when creating conditions for absolute synchronization of the frequency of pulsed light and vibrations of the vocal folds, instead of motionless vocal folds (as is normal), contractions or twitching in certain areas are visible, resembling trembling or flickering. In long-term severe forms of phonasthesia, leading to organic changes in the vocal folds, the absence of the phenomenon of displacement of the mucous membrane in the area of their anterior edge is typical.
Among organic dysphonias, the most common occupational diseases are chronic laryngitis and "singer's nodules". Contact ulcers of the vocal folds are quite rare among "voice professionals". The endoscopic picture of the listed diseases is typical. It should be noted that not only the above-mentioned diseases of the vocal apparatus are occupational, but also their complications and direct consequences.
Thus, the general otolaryngology concept of chronic laryngitis as a precancerous process provides grounds in a number of cases to consider a neoplasm of the larynx (in the absence of other etiological factors) professional if it developed in a patient - a “voice professional” who had a history of chronic inflammation of the vocal folds.
It should be noted that to date there are no specific objective criteria for the professional affiliation of vocal apparatus diseases, which sometimes leads to diagnostic errors and incorrect solutions to expert questions. In this regard, to determine the professional nature of a larynx disease, a thorough study of the anamnesis is necessary (excluding the impact of other etiological factors, primarily smoking, alcohol consumption, injuries, etc.; frequent visits to health care facilities for acute inflammatory diseases of the larynx or pharynx). Of decisive importance is the study of the sanitary and hygienic characteristics of working conditions in order to determine the degree of vocal load. The permissible norm of vocal load for persons in voice-speech professions is 20 hours per week. In addition, it is necessary to take into account the potentiating effect of concomitant factors of the surrounding production environment and the work process. Objective criteria are data from dynamic observation of the state of the upper respiratory tract, and primarily the larynx, using methods for determining the functional state of the larynx.
What do need to examine?
Who to contact?
Treatment vocal fold nodules
Treatment of patients with occupational diseases of the vocal apparatus is based on the principles of treatment of non-occupational inflammatory diseases of the larynx. In all cases of dysphonia, it is necessary to observe the voice regime and personal hygiene of the voice (excluding smoking, drinking alcohol), hypothermia should be avoided. Sanitation of foci of chronic infection is necessary.
Drug treatment
In organic diseases of the larynx, anti-inflammatory therapy, taking antihistamines, and instilling oils into the larynx are indicated. In vasomotor changes, a good therapeutic effect is provided by instilling oils into the larynx in combination with a suspension of hydrocortisone and ascorbic acid. In subatrophic processes, alkaline inhalations with vitamins and various biostimulants are useful; in hypertrophic forms, with zinc and tannin; in vasomotor diseases, with a suspension of hydrocortisone and procaine. Physiotherapeutic procedures are widely used: electrophoresis of the larynx with potassium iodide, potassium chloride, and vitamin E. In phonasthenia, additional sedative therapy is indicated (tranquilizers: diazepam, chlordiazepoxide, oxazepam, etc.). To increase vitality, these individuals are recommended to use extract of red deer antlers, ginseng extract, and eleutherococcus. Of the physiotherapeutic procedures for phonasthenia, hydrotherapy (rubbing with water, pine baths), gargling with sage and chamomile infusions have a good effect. To prevent relapses of phonasthenia, one should avoid overexerting the voice and various situations that negatively affect the nervous system.
Expertise of working capacity
The examination of both temporary and permanent loss of working capacity in occupational diseases of the vocal apparatus requires a special approach. Temporary impairment of working capacity in persons of voice and speech professions is discussed in the case when the pathological process that has arisen in the larynx is not long-term, reversible and after a short period of time the working capacity is fully restored. This can be the case with phonasthenia, injuries and hemorrhages in the vocal folds, that is, in the initial forms of occupational disease.
Temporary impairment of working capacity in persons of voice-speech professions is complete. This means that the worker is unfit for professional work for a short period, since any violation of the voice regime (silence regime) can aggravate the course of the disease he has.
Persistent impairment of working capacity in people with voice-speech professions often occurs during exacerbations of chronic laryngitis, recurrent phonasthenia, monochorditis and other laryngeal diseases. In these cases, the patient requires long-term inpatient treatment. In the absence of a positive clinical effect from the treatment, depending on the severity of the process and the functional state of the larynx, the patient is referred to the Medical and Social Expertise Commission to determine the degree of loss of working capacity. Such patients need to be monitored by a phoniatrist and otolaryngologist and undergo active treatment.
[ 14 ]
Prevention
Prevention of occupational diseases of the larynx should be based, first of all, on proper professional selection, teaching young specialists and students speech technique, instilling vocal hygiene skills. During professional selection, it is advisable to conduct a preliminary conversation with a psychoneurologist. Applicants should be sufficiently emotional, able to quickly react to the situation. The presence of foci of chronic infection in the upper respiratory tract is undesirable, after the sanitation of which it is necessary to re-solve issues of professional suitability.
Absolute contraindications for work in voice-speech professions are acute and chronic diseases of the larynx: chronic diseases of the pharynx of a dystrophic (especially subatrophic) nature, vasomotor and allergic reactions of the mucous membrane of the upper respiratory tract. A necessary condition for prevention is preliminary and periodic medical examinations.
It is advisable to conduct adapted health education work with consideration of issues regarding the necessary knowledge of speech technique, methods of using the vocal apparatus, and methods of autogenic training.