Medical expert of the article

New publications
Liver
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
The liver (hepar) is the largest gland, has a soft consistency, reddish-brown color. The length of the liver in an adult is 20-30 cm, width - 10-21 cm, height varies from 7 to 15 cm. The mass of the liver is 1400-1800 g. The liver is involved in the metabolism of proteins, carbohydrates, fats, vitamins; performs protective, disinfectant and other functions. In the uterine period, the liver is also a hematopoietic organ.
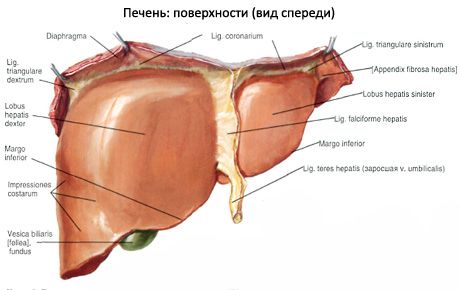
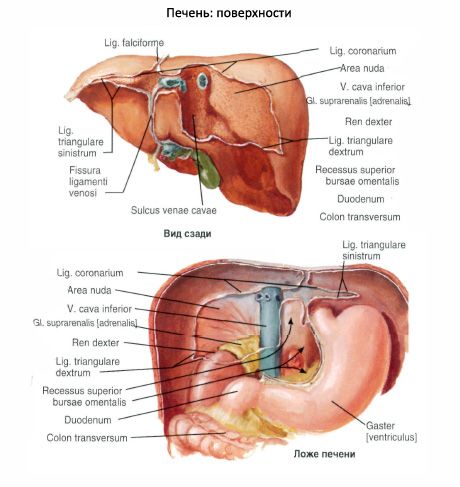
The liver has a diaphragmatic and visceral surface. The diaphragmatic surface (facies diaphragmatica) is convex, directed upward and forward. The visceral surface (facies visceralis) is flattened, directed downward and backward, its relief is uneven due to the internal organs adjacent to the liver.
In front, on the right and left, both surfaces of the liver converge.
The lower (anterior) edge of the liver (margo inferior) is sharp, the posterior edge of the liver is rounded.
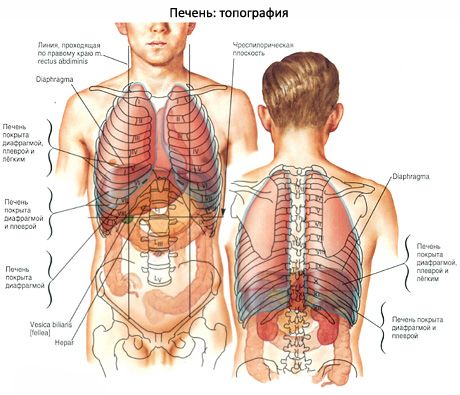
The liver is located in the right hypochondrium (mainly) and in the epigastrium. On the bones of the skeleton (on the ribs and spinal column) the liver is projected so that on the right and in front along the midclavicular line the highest point of the liver (right lobe) is determined at the level of the fifth intercostal space. The lower edge of the liver on the right along the axillary line is determined at the level of the tenth intercostal space. Then the lower border passes forward along the right costal arch. At the level of the right midclavicular line, the lower border of the liver is at the level of the costal arch, then goes from right to left and upward, crossing the epigastrium. At the level of the sixth left costal cartilage, the lower border (left lobe of the liver) crosses the costal arch and to the left of the sternum joins the upper border of the liver. Behind and on the right (along the scapular line) the border of the liver is at the level between the seventh intercostal space above and the upper edge of the eleventh rib below.

Above, the diaphragmatic surface is adjacent to the right and partially to the left dome of the diaphragm. In front, the liver in the upper part adjoins the costal part of the diaphragm and below - to the anterior abdominal wall. Behind, the liver is adjacent to the X-XI thoracic vertebrae, to the legs of the diaphragm, the abdominal part of the esophagus, the aorta, the right adrenal gland. Below, the liver is in contact with the cardiac part, the body and the pyloric part of the stomach, the upper part of the duodenum, the right kidney and the right adrenal gland, the right flexure and the right part of the transverse colon.
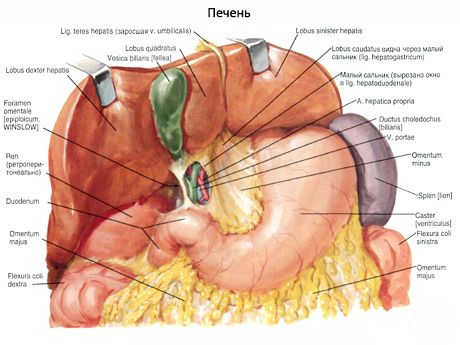
The surface of the liver is smooth, shiny, covered with peritoneum, with the exception of a small area on its posterior surface. The peritoneum, passing from the diaphragm to the liver, forms the so-called ligaments. The falciform ligament (lig.falciforme) of the liver, located in the sagittal plane, goes from the diaphragm and the anterior abdominal wall to the diaphragmatic surface of the liver. In the frontal plane is the coronary ligament (lig.coronarium), which connects to the posterior edge of the falciform ligament. On the sides, the coronary ligament forms expansions called the right and left triangular ligaments of the liver (lig.triangulare dextrum et lig.triangulare sinistrum). In the lower free edge of the falciform ligament is the round ligament of the liver (lig.teres hepatis), which has the appearance of a dense cord. It is an overgrown umbilical vein that connects the navel to the porta hepatis. From the porta hepatis to the lesser curvature of the stomach and to the initial part of the duodenum, two layers of peritoneum are directed, forming (on the left) the hepatogastric ligament (lig.hepatogastricum) and (on the right) the hepatoduodenal ligament (lig.hepatoduodenale).
On the diaphragmatic surface of the left lobe there is a cardiac indentation - a trace of the heart adjoining the liver (through the diaphragm).
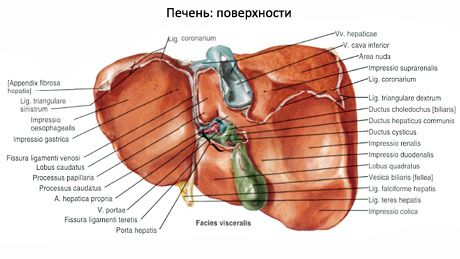
Anatomically, the liver is divided into two large lobes: right and left (lobus hepatis dexter et lobus hepatis sinister). The boundary between the larger right and smaller left lobes of the liver on its diaphragmatic surface is the falciform ligament of the liver. On the visceral surface, the boundary between these lobes is the groove of the round ligament of the liver in front, and the gap of the ligamentum venosum in the back, in which the ligamentum venosum is located, which is an overgrown venous duct that in the fetus connected the umbilical vein with the inferior vena cava.
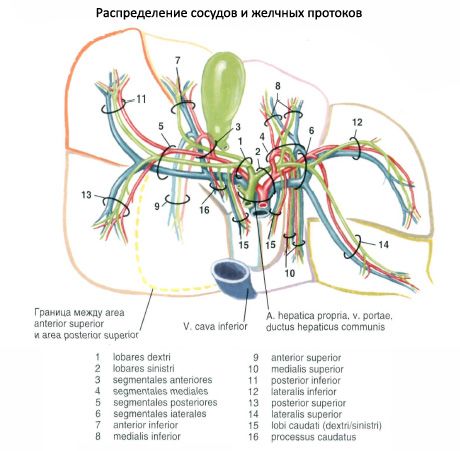
On the visceral surface of the liver, to the right of the groove of the round ligament and the fissure of the venous ligament, there is a right sagittal groove. Anteriorly, this groove widens and forms the fossa of the gallbladder (fossa vesicae biliaris, s.felleae), and posteriorly it forms the groove of the inferior vena cava (sulcus venae cavae). Between the right and left sagittal grooves there is a deep transverse groove called the porta hepatis. The porta hepatis is located at the level of the posterior edge of the fossa of the gallbladder and the fissure of the round ligament. The portal vein, proper hepatic artery, and nerves enter the porta hepatis; the common hepatic duct (sometimes the right and left hepatic) and lymphatic vessels exit.
On the visceral surface of the liver, within its right lobe, two small areas are distinguished: the square and caudate lobes. The square lobe (lobus quadratus) is limited on the left by the fissure of the round ligament, on the right by the fossa of the gallbladder, and behind by the porta hepatis. The caudate lobe (lobus caudatus) is located between the ligamentum venosum fissure on the left, the groove of the inferior vena cava on the right, and the porta hepatis in front. The caudate lobe has two processes. The caudate process (processus caudatus) is located between the porta hepatis and the groove of the inferior vena cava. The caudate process (processus papillaris) is also directed forward, it rests against the porta hepatis next to the fissure of the ligamentum venosum.
On the visceral surface of the liver there are impressions from contact with internal organs. On the visceral left surface there is a gastric impression (impressio gastrica). On the back of the left lobe there is an esophageal impression (impressio oesophagea). On the square lobe and in the area adjacent to the gallbladder fossa there is an impression of the duodenum (impressio duodenalis). To the right of it on the right lobe there is a renal impression (impressio renalis). To the left of the renal impression, next to the groove of the inferior vena cava, there is a suprarenal impression (impressio suprarenalis). On the visceral surface along the lower edge of the liver there is a colonic impression (impressio colica).
The liver is divided into 5 sectors and 8 segments. A sector is a section of the liver supplied with blood by a branch of the second-order portal vein and a branch of the proper hepatic artery, also of the second order. The sectoral bile duct emerges from a sector. A liver segment is a section of the liver corresponding to a branch of the third-order portal vein, from which the segmental bile duct emerges. The segments on the visceral surface are numbered in the direction from the groove of the inferior vena cava clockwise. Segments 1-4 are located in the left lobe, and segments 5-8 are located in the right lobe.

Liver lobes, sectors and segments
Share |
Sector |
Segment |
| Left lobe | Left dorsal | I (CI) |
| Left lateral | II (CII) |
|
| Left paramedian | Ш (СII) IV (CIV) |
|
| Right share | Right paramedian | V(CV), VIII (CVIII) |
| Right lateral | VI (CVI), VII (CVII) |

The left dorsal sector, corresponding to the first (CI) hepatic segment, includes the caudate lobe and is visible only on the visceral surface and posterior part of the liver.
The left lateral sector (segment II - CII) covers the posterior part of the left lobe of the liver.
The left paramedian sector occupies the anterior part of the left lobe of the liver (segment III - CIII) and its square lobe (segment IV - CIV) with a parenchyma area on the diaphragmatic surface of the organ in the form of a strip that narrows posteriorly (towards the groove of the inferior vena cava).
The right paramedian sector is the liver parenchyma bordering the left lobe of the liver. This sector includes segment V (CV), which occupies the posteromedial part of the right lobe of the liver on its diaphragmatic surface.
The right lateral sector, corresponding to the most lateral part of the right lobe of the liver, includes segments VI-CVI (lies in front) and VII-CVII. The latter is located behind the previous one and occupies the posterolateral part of the diaphragmatic surface of the right lobe of the liver.
From the fibrous capsule, layers of connective tissue extend deep into the liver, dividing the parenchyma into lobules, which are the structural and functional units of the liver.
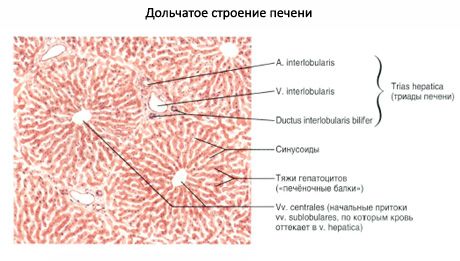
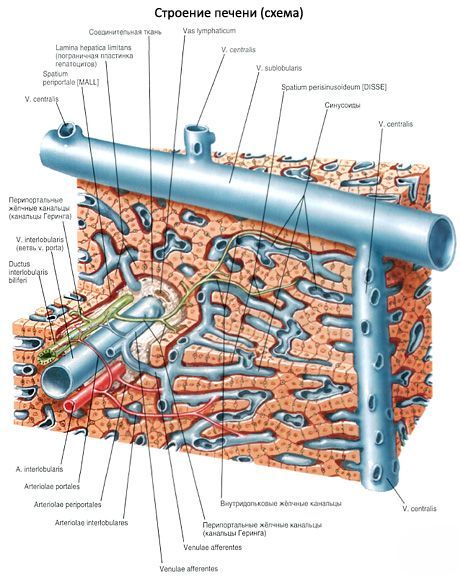
The liver lobule (lobulus hepatis) has a prismatic shape, its diameter is 1.0-1.5 mm. The total number of lobules is approximately 500 thousand. The lobule is built from radially converging from the periphery to the center of cell rows - liver beams. Each beam consists of two rows of liver cells - hepatocytes. Between the two rows of cells within the liver beam are the initial sections of the bile ducts (bile ducts, ductulus bilifer). Between the beams are radially located blood capillaries (sinusoids), which converge from the periphery of the lobule to its central vein (v. centralis), located in the center of the lobule. Between the wall of the sinusoidal capillary and the hepatocytes there is a perisinusoidal space (Disse). Between the lobules there is a small amount of connective tissue, in the thickness of which are located interlobular bile ducts, arteries and veins. The interlobular ducts, artery and vein are located next to each other, forming the so-called liver triad. Due to this structure, hepatocytes secrete bile in two directions: into the bile ducts - bile, into the blood capillaries - glucose, urea, fats, vitamins, etc., which entered the liver cells from the bloodstream or formed in these cells.

Hepatocytes have a polygonal shape, their diameter is 20-25 μm. Most hepatocytes have one nucleus, a smaller part - two or more nuclei. The cytoplasm of the hepatocyte looks large- or small-celled depending on the expression and composition of inclusions (lipids, pigments). Hepatocytes have many mitochondria, pronounced endoplasmic reticulum and Golgi complex, a significant number of ribosomes, lysosomes, and microbodies with products of fatty acid metabolism. There are many glycogen grains in the cytoplasm. The cytolemma of hepatocytes has numerous microvilli facing the perisinusoidal space, towards the blood capillaries.
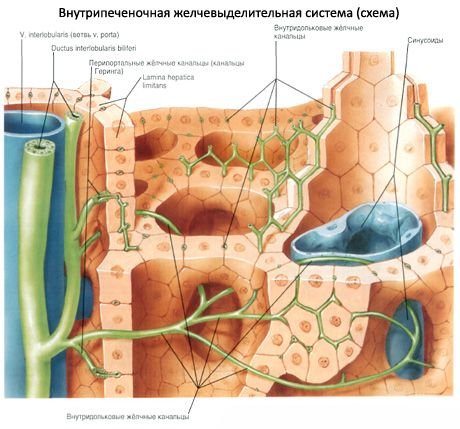
The bile ducts originate from the intrahepatic lobules.
The liver lobules contain bile ducts, or canaliculi. The lumen (diameter) of the bile ducts is 0.5-1 µm. They do not have their own walls, since they are expanded zones of intercellular gaps between the rows of hepatocytes that make up the liver trabecula. The bile ducts have short blind branches (intermediate canaliculi of Hering), which enter between adjacent hepatocytes that form the walls of the bile ducts. The bile ducts (canaliculi) begin blindly near the central vein and go to the periphery of the lobule, where they open into interlobular (perilobular) bile ducts (ductuli interlobulares). The interlobular ducts connect with each other, increase in diameter, and form the right and left hepatic ducts (ductus hepaticus dexter et sinister). At the porta hepatis, these two ducts join to form the common hepatic duct, 4-6 cm long. Between the layers of the hepatoduodenal ligament, the common hepatic duct joins with the cystic duct (duct of the gallbladder) and forms the common bile duct.
The common bile duct (ductus choledochus, s.biliaris) is located between the layers of the hepatoduodenal ligament, in front of the portal vein and to the right of the proper hepatic artery. Then the common bile duct goes behind the upper part of the duodenum, then between its descending part and the head of the pancreas. In the wall of the duodenum, the common bile duct joins the pancreatic duct and together with it forms an expansion - the hepatopancreatic ampulla (ampulla hepatopancreatica). The ampulla opens into the duodenum at the apex of its major papilla. In the walls of the mouth of the hepatopancreatic ampulla there is a thickening of circular bundles of myocytes that form the sphincter of the hepatopancreatic ampulla, or sphincter of Oddi. The distribution of circular smooth muscle bundles of this sphincter is uneven. Smooth muscle bundles are most concentrated at the base of the large papilla and have a thickness of up to 75 μm, in the thickness of the papilla itself - 40 μm. The length of the sphincter is 15-20 μm.
Between digestion processes, the sphincter of Oddi is closed, bile accumulates in the gallbladder, where it is concentrated. During the digestion process, the sphincter of Oddi opens and bile enters the duodenum.
There is also a sphincter in the walls of the terminal part of the common bile duct before it merges with the pancreatic duct. This sphincter of the common bile duct, when contracted, blocks the flow of bile from the bile ducts into the hepatopancreatic ampulla and then into the duodenum.
The walls of the interlobular bile ducts are formed by a single-layer cuboidal epithelium. The walls of the hepatic, cystic and common bile ducts have three membranes. The mucous membrane is lined with a single-layer high prismatic epithelium. The epithelium also contains goblet cells. The proper plate of the mucous membrane is well developed, contains many longitudinal and circular elastic fibers, a few multicellular mucous glands. The submucosa is poorly developed. The muscular membrane is thin, consists mainly of spiral bundles of smooth myocytes, between which there is connective tissue.
Innervation of the liver
The liver is innervated by branches of the vagus nerves and the hepatic (sympathetic) plexus.
Blood supply to the liver
The hepatic portal artery and portal vein enter the porta hepatis. The artery carries arterial blood, and the portal vein carries venous blood from the stomach, pancreas, intestines, and spleen. Inside the liver, the artery and portal vein branch into interlobular arteries and interlobular veins, which are located together with the bile interlobular ducts between the liver lobules. From the interlobular veins, wide blood capillaries (sinusoids) branch off into the lobules, flowing into the central vein. Arterial capillaries flowing from the interlobular arteries into the initial sections of the sinusoids. The central veins of the liver lobules connect with each other, forming sublobular (collecting) veins. The sublobular veins merge with each other, become larger, and ultimately form 2-3 hepatic veins. They exit the liver in the region of the groove of the inferior vena cava and flow into this vein.
Lymph drainage: to the hepatic, celiac, right lumbar, upper diaphragmatic, parasternal lymph nodes.
 [ 3 ], [ 4 ], [ 5 ], [ 6 ], [ 7 ]
[ 3 ], [ 4 ], [ 5 ], [ 6 ], [ 7 ]
Age-related features of the liver
In a newborn, the liver is large and occupies more than half of the abdominal cavity. The liver mass in a newborn is 135 g, which is 4.0-4.5% of the body weight (in adults 2-3%). The diaphragmatic surface of the liver is convex, the left lobe of the liver is equal in size to the right or larger. The lower edge of the liver is convex, under its left lobe is the colon. The upper border of the liver along the right midclavicular line is at the level of the 5th rib, and along the left - at the level of the 6th rib. The left lobe of the liver crosses the costal arch along the left midclavicular line. The transverse size of the liver in a newborn is 11 cm, longitudinal - 7 cm, vertical - 8 cm. In a child of 3-4 months, the intersection of the costal arch with the left lobe of the liver, due to a decrease in its size, is already at the parasternal line. In newborns, the lower edge of the liver along the right midclavicular line protrudes from under the costal arch by 2.5-4.0 cm, and along the anterior midline - by 3.5-4.0 cm below the xiphoid process.

Sometimes the lower edge of the liver reaches the wing of the right ilium. In children aged 3-7 years, the lower edge of the liver is 1.5-2.0 cm below the costal arch (along the midclavicular line). In a 7-year-old child, the liver weighs 700 g. After 7 years, the lower edge of the liver does not extend from under the costal arch; only the stomach is located under the liver. From this time on, the skeletotopy of the child's liver is almost no different from the skeletotopy of an adult. In children, the liver is very mobile, and its position easily changes with a change in body position. The liver reaches its final size after 20-29 years. After 60-70 years, the liver's weight decreases, its connective tissue grows. With age, the amount of lipofuscin in hepatocytes increases, the number of dividing hepatocytes decreases sharply, and the size of their nuclei increases.
[ 8 ], [ 9 ], [ 10 ], [ 11 ], [ 12 ], [ 13 ], [ 14 ], [ 15 ]