Medical expert of the article

New publications
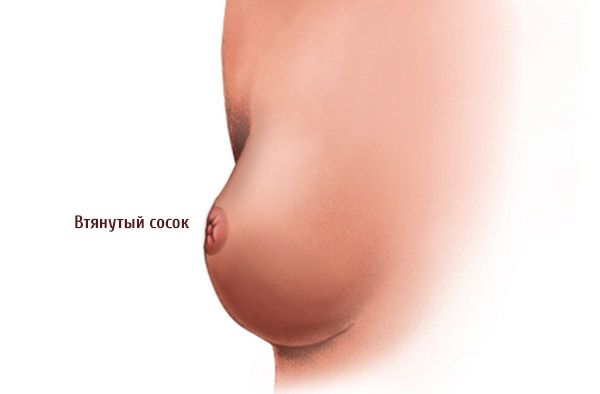
Retracted nipple
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

This pathology occurs in every tenth woman. And, as a rule, a flat or inverted nipple worries women most, either as an element of aesthetic imperfection, or when lactation begins after childbirth and a young mother faces the problem of how to feed a newborn. In this case, mammologists distinguish two types of this anatomical deviation: when an inverted nipple hardens and becomes convex after manual stimulation and the inversion variant - a truly inverted state. This article mostly aims to highlight the more severe second case of pathology.
Causes retracted nipple
Many women, faced with this problem, acquire an inferiority complex, asking the question, why did this happen? The reasons for such a clinical picture can be different.
- Heredity.
- Incorrect selection of a bra. This is especially common if a woman wants to visually reduce her breasts by using a deliberately smaller size than necessary. Or incorrect selection of the size and model of the bra.
- Diseases affecting breast tissue.
- Congenital abnormality of the connective tissue that holds the milk ducts.
- Disruption of the period of sexual development of a girl - insufficient formation of milk ducts and mammary glands.
- Tumor formations (both benign and malignant).
These reasons make the nipple to be drawn into the areola. This situation not only causes aesthetic discomfort to the woman, but is also dangerous. It can become a risk factor for the development of an inflammatory process in the breast - mastitis.
 [ 1 ]
[ 1 ]
Symptoms retracted nipple
To speak more confidently about the type of nipple, you should conduct a simple test. Its essence is as follows: take the nipple at its base with your thumb and index finger and gently squeeze. If it moves outward even more - the natural state of the norm, and if it goes inward - retracted.
The main symptoms of an inverted nipple are quite visual - the nipple is constantly either at the same level as the areola, or completely “sunk” inward.
Such an anatomical picture is an anomaly and requires a specialist consultation. In this case, it will be a mammologist.
Today, doctors divide this pathology into two types:
- Hidden. When the nipple swells freely enough during manual stimulation and does not cause much discomfort when feeding the baby.
- Inverted. A situation when the nipple is always located inside the areola. This situation does not change with manual stimulation. It is this pathology that causes the woman the greatest troubles and problems, both aesthetic and functional.
Women who have an abnormality in the structure of the breast, namely the inverted nipple variant, often complain of pain in this area of the body. Basically, such symptoms accompany them during the period of breastfeeding the newborn.
Due to its incorrect structure, such a nipple does not allow the baby to grasp it normally. The child tries to do this as best he can, but at the same time he causes pain to the mother with his actions. Another reason for the pain in this situation is the incorrect use of the "attachment" - an artificial nipple.
Therefore, if the nipple is drawn in and hurts, it is advisable to consult a specialist. Perhaps the cause of discomfort is one of the reasons listed above, or perhaps the young mother simply chose the wrong position for feeding her baby.

Complications and consequences
An inverted nipple often creates aesthetic discomfort for a woman, developing an inferiority complex.
Over time, the consequences of such a deviation from the norm lead to other problems. And the most significant of them a woman faces immediately after childbirth.
[ 2 ], [ 3 ], [ 4 ], [ 5 ], [ 6 ]
Complications
This deviation refers to a pathology of psychological, cosmetic, and, most importantly, physiological nature. If we talk about the consequences for the patient's health, then any pathological changes do not threaten her.
But there are clinical situations when a woman is offered correction of a pathological defect by means of surgical intervention. When going for surgery, the patient must be prepared for the fact that complications are possible in the postoperative period, which will have to be stopped.
Such consequences may include:
- Swelling around the surgical tissues.
- Pain at rest or when touched.
- Skin irritation.
- Allergic reaction to a drug or material.
- Infection with subsequent suppuration of the wound.
- Development of hematoma.
- Formation of scars.
If the operation is performed correctly, these symptoms will pass fairly quickly.
Diagnostics retracted nipple
The inverted nipple is perfectly visualized. And this is the first thing that catches the eye when examining the mammary glands. Subsequent diagnostics of this problem may consist of the doctor prescribing additional laboratory tests and instrumental diagnostics.
- Blood and urine tests are required.
- Visual examination of the mammary glands and areas of localization of nearby lymph nodes. In this case, it is the axillary area.
- Cytology of material taken from the surface of the nipple.
- Radiography.
- Ultrasound examination of the area of interest.
- If necessary, X-ray diagnostics of soft tissues in the axillary area.
Instrumental diagnostics
- Ultrasound examination of the mammary glands (ultrasound).
- Color Doppler mapping (CDM).
If necessary, additional examination may be prescribed. This may include:
- Laser mammography.
- Magnetic resonance imaging.
- When planning surgical treatment, a woman is offered (if possible) a panoramic sonography.
- Multislice computed tomography of the mammary glands with intravenous contrast enhancement.
- Aspiration biopsy performed under monitoring by means of radiological and ultrasound techniques.
- Three-dimensional ultrasonography – performing an ultrasound examination in 3D format.
- Radionuclide diagnostics is an analysis of parameters obtained after the introduction of special biochemical or chemical compounds into the patient’s body.
- Examination of tumor markers (in case of suspected breast cancer).
- Chest phlebography, if there is a suspicion of damage to the axillary lymph nodes.
Who to contact?
Treatment retracted nipple
There are two main methods of treating an inverted nipple: surgical and non-surgical. Depending on the nature of the pathology, normalization of the nipple shape can occur through radical intervention in the structure of the nipple and, through plastic surgery, giving it new shapes.
Non-surgical therapy includes a number of methods. These may include:
- Treatment by performing a specific set of exercises.
- Correction of the inverted nipple defect using a cup-shaped vacuum attachment.
- Using nipple shields.
The choice of option largely depends on the woman herself. Before deciding on the operation, she should answer the following question: does she plan to become pregnant and breastfeed the newborn? If so, then the surgical intervention makes sense. The woman's desire to correct the defect for the sake of aesthetic correction can lead to the same result.
What to do if you have an inverted nipple?
As statistics show, approximately ten percent of women face the problem we are considering in this article. Therefore, the question of what to do with an inverted nipple is quite relevant for them and requires immediate clarification.
As already mentioned above, before trying to solve the problem on your own, it would be a good idea to consult a specialist (mammologist). He, having conducted the appropriate examinations, will differentiate the problem and suggest ways to solve it.
If there are indications, a woman is planning a pregnancy and wants to breastfeed her baby on her own, and her health allows it, you can use surgical nipple plastic surgery. This radical method will solve the existing problem once and for all.
The specialist can also offer the patient the most suitable method for her case of non-surgical solution of the pathological deviation. She will be offered a set of special exercises or the use of pads specially designed for such pathology during feeding.
The set of exercises mainly comes down to manual stimulation of the nipple with the phalanges of the hands. These actions are aimed at forming an adequate reaction of the nipple to irritation. This technique is most effective in case of false convexity, when stimulation leads to the nipple swelling and taking up space, rising above the areola ring.
The essence of the exercise is rhythmic squeezing of the base of the nipple with two fingers (index and thumb), first inward, and then making rhythmic movements, as if pulling the nipple out. This procedure should be performed for several minutes two to three times a day for two to three months.
It should be noted that this stimulation is absolutely unacceptable during the period when a woman is pregnant and is in the first or second trimester. Since stimulation of the nipple also contributes to an increase in the tone of the uterus, which can cause premature birth, and as a result - the loss of the child and termination of pregnancy.
Surgical treatment
One of the methods that helps resolve the existing anatomical deviation is surgical treatment, which the doctor can resort to either at the patient's request or at the doctor's insistence if this pathology becomes an obstacle for the woman in terms of breastfeeding her baby. In any case, there must be voluntary consent of the patient and the absence of contraindications to surgical intervention.
This method makes it possible to solve this issue radically and quite quickly. Today, there are several methods of surgical intervention. The choice largely depends on the answer to the question of whether the woman plans to give birth and breastfeed the newborn in the future.
To understand the essence of surgical treatment, it would be useful to recall the structure of the area of interest to us. Approximately 25 milk ducts have their outlet on the nipple surface. At the same time, they are supported and connected to each other by strands of connective fibers, the other end of which is fixed in the deep layers of the mammary gland. If these connective fibers are smaller than necessary, the picture considered in this article is obtained.
The simplest option is to intersect the milk ducts, which, being shorter than expected or suffering from loss of elasticity, are under tension and do not allow the nipple to rise above the areola.
The second operation makes it possible to preserve the milk ducts intact.
The operation preserving the milk ducts can be performed under either general or local anesthesia. In this case, organ-preserving surgery can also be performed in two ways:
- When only the nipple and areola are directly subject to correction.
- In parallel with the manipulations of the first point, the surgeon-mammologist also performs mammoplasty. That is, a lift, increase or decrease in the size of the breast is performed.
In this case, a small incision (up to 1 cm in size) is made at the base of the areola, through which the specialist performs the necessary manipulations under the control of a microscope. This procedure usually takes about an hour.
The consequences of the operation in the postoperative period may be:
- The appearance of a hematoma.
- Swelling of the operated area.
- Decreased nipple sensitivity.
But usually, within the first week after surgery, swelling and bruising subside, and sensitivity is restored.
During the following month, a woman who has undergone surgery must take care of herself:
- Avoid lifting heavy weights and strenuous physical activity.
- You shouldn't wear tight underwear.
- Prefer natural materials in clothing and bed linen.
- Avoid visiting swimming pools, solariums, open water bodies, and sunbathing outdoors.
The consequences of such surgical intervention remain virtually unnoticeable.
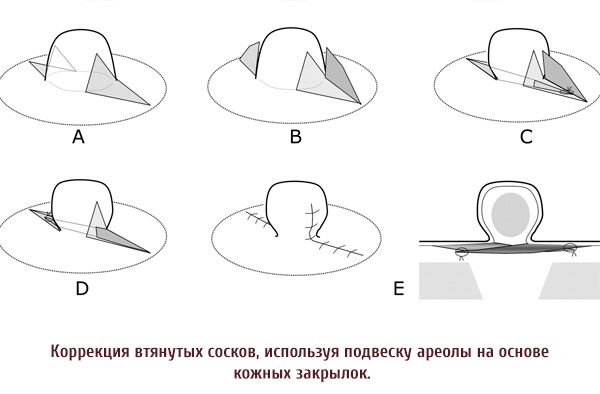
Correction of inverted nipples
Modern medicine is ready to offer women with an anatomical defect of the breast in the form of an inverted nipple, a non-surgical solution to the problem. In this regard, doctors can offer a number of devices, thanks to the use of which the correction of inverted nipples occurs. Such methods include stimulation of the nipple with a vacuum, as well as the use of special corrective caps that allow you to replenish the missing volume of the nipple.
Inverted nipple corrector
One of the devices that allows you to partially or completely solve the problem during feeding your baby is a corrector for inverted nipples. This device is a modifier that repeats the shape of the areola and the nipple itself. This device is used during lactation.
Before feeding, the woman fixes the cap-corrector on the breast. It prevents the nipple from being drawn in during the period when the newborn is being fed. At the same time, the cap-corrector plays the role of protection against the formation of cracks on the nipple and surrounding tissues.
The essence of the method is in forced stretching of the milk ducts to their natural size. This allows to remove the feeding problem and makes it possible to easily establish lactation.
Vacuum attachments for inverted nipples
This device was developed by the English plastic surgeon Douglas Mac George. Vacuum attachments for inverted nipples are becoming increasingly popular among women who have encountered this problem.
Made from hypoallergenic material, such as silicone, the vacuum nozzle is easy to use. But the effectiveness of its use varies from case to case. If the nipple falls into the areola, while during stimulation it takes its natural place, then this technique, with regular use, after three to four weeks will solve the problem and return the nipple to its normal position.
If the nipple is pathologically retracted, then such a significant result cannot be expected, but its use will make it possible, in this case, to normalize feeding.
The mechanism of the corrector is simple and is based on the phenomenon of vacuum. A specially made cap is put on the nipple. Using a check valve, a syringe is connected to it, with the help of which air is pumped out of the internal area, creating a vacuum in this area. After disconnecting the syringe, the vacuum is maintained thanks to the check valve. Under the action of the vacuum, the inverted nipple is stretched, acquiring a natural shape.
If you wear this device daily for eight hours, then after three to four weeks the nipple will begin to hold its natural shape on its own. This result is achieved due to the soft and measured stretching of the tissue structures of the milk ducts that hold the nipple in a certain abnormal position. The use of this device does not cause any significant negative impact on the main functions of the breast.
But it is worth noting that this result is possible only in the case of false nipple retraction. If a woman is diagnosed with a truly inverted nipple, then this method will not lead to significant changes in the situation.
Vacuum attachments for inverted nipples on the shelves of modern pharmacies today are presented in a variety of modified versions, allowing a woman to independently choose the model that suits her best.
A nipple shaper is usually worn inside the bra cups for a minimum of eight hours (day and/or night).
Clinical trials have shown the high effectiveness of this method of relieving the problem.
How to feed a baby with inverted nipples?
If a woman has an inverted nipple, it is advisable to correct it before planning a pregnancy. If such "treatment" has not been carried out, then over time the question arises: how to feed a child with inverted nipples?
In such a situation, experts advise preparing nipples for the lactation period, starting from the 38th week of pregnancy. Preparing inverted nipples for feeding a child consists of a whole range of measures that allow you to solve the problem before lactation begins.
These methods include massage or, as it is also called, "special exercises for normalizing an inverted nipple." The essence of the exercise is rhythmic compression of the base of the nipple with two fingers (index and thumb), first inward, and then making rhythmic movements, as if pulling the nipple out. This procedure should be performed for several minutes (no more than ten) two to three times a day for two to three months. When performing this exercise, it is advisable to apply a thin layer of lanolin or massage oil to the areola. This will protect the sensitive skin of the breast from physical damage and will allow you to perform the exercise correctly.

Feeding with inverted nipples
You should be prepared right away that the first attachment to the breast will be problematic.
A woman will have to be patient and work hard to establish lactation and feeding in such a situation.
Will try to figure out what needs to be done in this case to quickly solve the problem.
- The first thing that can be advised to such women is the position during feeding. During the feeding period, the young mother should take the baby in her arms and slowly walk around the room. This move will help develop the sucking reflex in the newborn. After all, this position is familiar to him, he felt it for nine months while in the womb.
- It is necessary to choose the right feeding position. This applies to both the baby and the mother. The baby's head should be positioned so that its mouth is parallel to the nipple. To achieve this, the mother should hold the baby in one hand, and support the breast with the other.
- Before you start feeding, you need to get advice on how to properly hold the fingers of the hand that is placed on the chest. The four phalanges should support the chest from below, and the phalanx of the thumb fixes the chest from above.
- When feeding while standing, it is advisable to protect the baby. To do this, you should swaddle him or put him in a sling. In such a situation, the baby is deprived of the opportunity to actively move, which will somewhat facilitate the feeding procedure.
- If the baby fails to take the nipple into his mouth the first time. Do not force it there. Such "violence" will only push the baby away, reinforcing the negative perception. It is worth trying to slightly tease the baby by moving the nipple over his lips. Reflexively, the child will join the game and try to grab the nipple.
- In order for the baby to not have such a hard time grasping the inverted nipple with his lips at first, it is necessary to express a small amount of breast milk before each feeding. This will relieve tension in the breast and make it softer and more pliable. In this situation, it is necessary to present the nipple together with the areola.
To help yourself with breastfeeding with inverted nipples, a woman should consult with her doctor, who will help her choose a device that will make it easier to cope with the problem. Fortunately, the modern market is ready to offer a fairly good selection of models, both corrective caps (silicone pads) and special vacuum attachments.
Inverted Nipple Piercing
Modern piercing has found a second wind. Where only, and on what parts of the body, do you not see these "works of art". But in light of the pathology we are considering, we will try to illuminate it from this side.
In social networks, many respondents who have had to deal with this problem are wondering whether it is possible to get a piercing on inverted nipples? And whether this procedure can correct the situation by pulling the nipple out and making it naturally normal.
As experience has shown, there is a grain of truth in these assumptions. In some cases, a nipple piercing, to some extent, replaces a vacuum, “pulling” the nipple to a normal position. And it works.
But you shouldn't rush to do this procedure to solve the problem without looking back, since it is still an injury to the nipple with an open wound. And if the puncture is not done by a professional and in unsanitary conditions, then such "treatment" will not lead to anything good.
The procedure itself, as already mentioned, must be carried out in sterile conditions by a professional.
In some cases, it is simply technically impossible to pierce the nipple, precisely because the nipple is retracted. So it is not that simple.
Prevention
There are currently no specific measures that can prevent the development of an inverted nipple. This prevention comes down to timely detection, diagnosis and treatment of diseases and pathological anatomical deviations that can lead a woman's breast to pathology associated with a change in the position of the nipple.
Forecast