
Rheoencephalography
Last reviewed: 23.04.2024

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Rheoencephalography (REG) is based on the measurement of changes in the impedance of the head associated with the pulse wave when a weak high-frequency electric current passes through the electrodes. Since this resistance largely depends on the blood filling of tissues, one of the synonyms of the REG method is "impedance electroplethysmography" (although it is often used for methods of measuring slower impedance oscillations - on the order of tens of seconds or minutes).
The period of the REG wave depends on the heart rate, whereas its amplitude parameters are predominantly (by 90%) due to changes in the intracranial blood filling and reflect the state of the intracerebral vessels (especially in the basilar carotid artery ).
 [
[The purpose of carrying out rheoencephalography
The aim of the REG is to detect abnormalities in the blood supply to the brain (especially the blood flow in the basins of large and medium cerebral vessels) and intracranial hypertension to exclude or evaluate the contribution of the "vascular" factor to psychopathological and neurologic symptoms.
How is rheoencephalography performed?
On the scalp impose 2-6 electrodes, fixed with rubber bands, strips or adhesive compounds. To prevent polarization, the electrodes are coated with a special non-polarizing coating (Ag-AgCl) and a weak (1-10 mA) alternating current with a frequency of 30-150 kHz is used. The electrodes are placed on the frontal, occipital region and on the mastoid process on each side.
Frontal-mastoid ducts reflect blood filling mainly in the basin of the middle cerebral artery, and mastoid-occipital leads in the intracranial part of the basin of the vertebral artery.
Registration of the rheoencephalogram
The REG recording device (rheograph) includes a high frequency current generator, a measuring bridge, an amplifier, a detector and a recording device. In modern devices, a multiplexer amplifier is used to unify amplification over several channels and a computer for automatic calculations of quantitative parameters and visualization of the results (including in the form of schematic maps of blood filling).
Interpretation of results
Normal rheoencephalogram
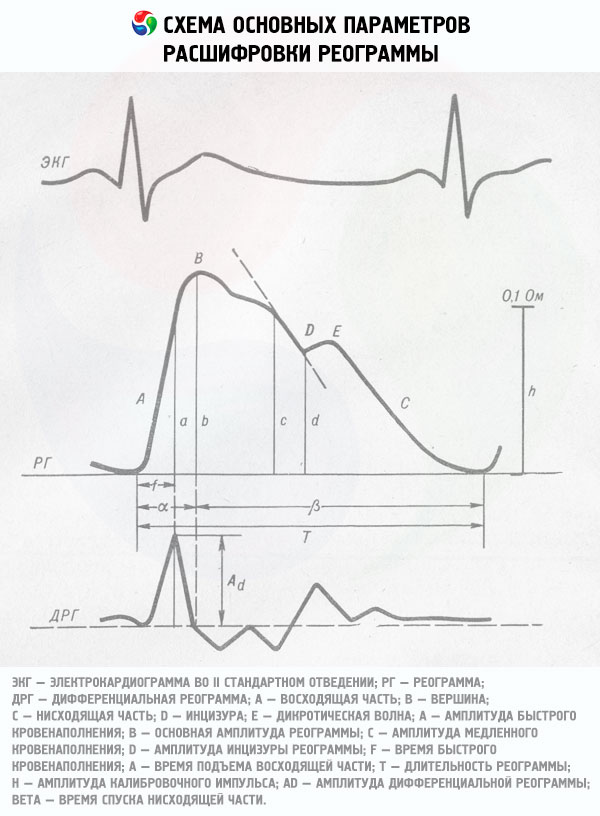
Rheogram in shape resembles pulsogram. In the single wave of REG, the beginning, the vertex (systolic wave) and the end are distinguished. The section of the curve from the beginning to the top is called the ascending (anacrotic) part, the portion from the top to the end of the wave is the descending (cataract) part. Normally, the ascending part is shorter and steeper, and the descending part is longer and more sloping. In the descending part, as a rule, one additional wave (a dicrotic prong) is identified, consisting of a depression and a vertex. This complex is called a diastolic wave.
Rheoencephalogram in pathology
Since the configuration of the components of the wave REGG is largely due to the reflection of the pulse wave from the branching points of the arteries, as well as the elasticity and tone of the vessel wall, from the change in the shape of the REG it is possible to judge certain violations of the cerebral blood flow.
With an increase in the vascular tone, the amplitude decreases and the systolic wave tops up, the additional (diastolic) wave shifts toward the apex, and the depression decreases. When the vascular tone decreases, on the contrary, the amplitude and sharpening of the systolic wave increase, the intensity of the additional wave increases, and its shift toward the end of the REG wave.
When the venous outflow obstructs, the REG wave flattenes, becomes dome-shaped, and with venous hypotension a small presystolic wave appears before the onset of the systolic wave.
The software of modern computer rheographs allows to automatically measure the above-mentioned amplitude-time parameters of the REG wave and also to calculate a number of special indices describing the relationships between them that are more informative for assessing the tone and resistance of large, medium and small arteries and veins than the absolute values of REG parameters .