Medical expert of the article

New publications
Kidney dysplasia
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Renal dysplasia occupies a prominent place among the developmental defects of the urinary system. Renal dysplasia is a heterogeneous group of diseases associated with impaired renal tissue development. Morphologically, dysplasia is based on impaired differentiation of the nephrogenic blastema and branches of the ureteral sprout, with the presence of embryonic structures in the form of foci of undifferentiated mesenchyme, as well as primitive ducts and tubules. Mesenchyme, represented by pluripotent cambial cells and collagen fibers, can form dysontogenetic derivatives of hyaline cartilage and smooth muscle fibers.
 [ 1 ]
[ 1 ]
Causes renal dysplasia
Pathogenesis
Morphological examination of hypoplastic dysplasia reveals some decrease in kidney mass, a lobular surface, not always clearly defined division into layers, sometimes some expansion or hypoplasia of the ureters. Microscopically, primitive structures are detected: many glomeruli are reduced in size, vascular loops are atrophic, the capsule is thickened. The shape of the glomeruli can be S-shaped or ring-shaped, many of them are hyalinized and sclerosed. The glomeruli are arranged in a grape-like manner, surrounded by loose connective tissue with focal accumulations of lymphoid and histiocytic cells. In the medulla, there are many primitive ducts and tubules, which are immature formations of various stages of embryonic development. Primitive ducts are mainly detected in the juxtamedullary zone and are the remains of the mesonephrogenic duct. A characteristic feature is the presence of shadows of smooth muscle cells and connective tissue fibers around them. The presence of primitive structures reflects a delay in the maturation of the nephron.
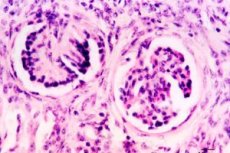
Morphological examination of simple focal dysplasia does not reveal any significant changes in kidney mass. In some cases, a decrease in the cortex thickness is observed. This nephropathy is diagnosed based on histological changes revealed by microscopy. Simple focal dysplasia is characterized by the presence of clusters of primitive glomeruli and tubules, surrounded by connective tissue fibers and smooth muscle cells, mainly in the renal cortex; sometimes cartilaginous tissue is found. Polymorphism of the epithelium of convoluted tubules is characteristic, where adjacent cells differ in size, configuration, set and number of intracellular organelles. Some children may have dilated tubular lumens in the kidneys. Glomerular cysts may also be detected, but their number is insignificant. Mesenchymal mononuclear cells are determined in the stroma.
Simple segmental dysplasia (Ask-Upmark kidney) is quite rare (0.02% of all autopsies). In this type of dysplasia, the kidney is reduced in size, a transverse groove is clearly visible on the outer surface at the site of the hypoplastic segment, and the number of pyramids is reduced. Morphological changes are caused by dysembryogenesis of vessels in individual segments of the kidney with subsequent disruption of differentiation of tissue structures due to changes in the blood supply to these areas. Underdevelopment of the corresponding arterial branches is usually detected. A characteristic feature is the presence of primitive mesonephrogenic ducts in the hypoplastic segment, surrounded by smooth muscle cells and foci of hyaline cartilage. In addition, sclerosis, glomerular hyalinosis, atrophy of the tubular epithelium with expansion of their lumen, signs of fibrosis and cellular infiltration, and interstitium develop.
Aplastic cystic dysplasia (multicystic rudimentary kidney) accounts for 3.5% of all congenital malformations of the urinary system and 19% of all forms of cystic dysplasia. The kidneys are significantly reduced in size, are shapeless formations of cysts 2-5 mm in diameter, the renal parenchyma is almost completely absent, the ureter is absent or atresia is present. Microscopically, a large number of cysts are detected, both glomerular and tubular, as well as primitive ducts and foci of cartilaginous tissue. Bilateral damage is incompatible with life. Unilateral rudimentary kidney is often detected during a random examination, and the second kidney is often abnormal.
Hypoplastic cystic dysplasia (multicystic hypoplastic kidney) accounts for 3.9% of all urinary system defects and 21.2% of cystic dysplasias. The kidneys are reduced in size and weight. Glomerular cysts are usually located in the subcapsular zone, their diameter varies and can reach 3-5 mm. Tubular cysts are found both in the cortex and in the medulla. Connective tissue fibrosis and the presence of primitive ducts are more significant in the medulla. The cysts are large and represent cystically dilated collecting tubules. The renal parenchyma is partially preserved. Between the pathologically altered areas there are collecting tubules of normal structure. The renal pelvis may be unchanged, more often hypoplastic, as is the ureter. Hypoplastic cystic dysplasia is often associated with defects of the lower urinary tract, gastrointestinal tract, cardiovascular system and other organs.
Bilateral damage leads early to the development of chronic renal failure. As a rule, with a unilateral variant of this dysplasia, the second kidney has some manifestations of dysembryogenesis.
Hyperplastic cystic dysplasia often accompanies Patau syndrome. The process is bilateral. The kidneys are enlarged in size, covered with multiple cysts. Microscopic examination reveals primitive ducts, cysts in large numbers in the cortex and medulla. Lethal outcome usually occurs at an early age.
Multicystic dysplasia (multicystic kidney) is a developmental defect in which the kidneys are enlarged in size, there is a large number of cysts of various shapes and sizes (from 5 mm to 5 cm), between which the parenchyma is practically absent.
Microscopy reveals primitive ducts and glomeruli between the cysts, and areas with cartilaginous tissue may also be encountered. In case of bilateral lesions, death occurs in the first days of life. In case of unilateral lesions, the diagnosis is made by chance during palpation of a tuberous tumor-like formation or based on ultrasound results. In case of unilateral multicystic disease, there may be malformations on the part of the second kidney (often hydronephrosis), heart defects, gastrointestinal tract defects, etc.
In medullary dysplasia (cystic dysplasia of the medulla, medullary cystic disease, Fanconi nephronophthisis), the kidneys are usually reduced in size, often retaining embryonic lobulation. The cortex is thinned, the medulla is expanded due to a large number of cysts up to 1 cm in diameter, including characteristic cystic expansion of the collecting ducts. Microscopy reveals a decrease in the size of many glomeruli, some of them are hyalinized and sclerotic, the interstitium is also sclerotic, and there is lymphoid infiltration in the stroma.
A special place among cystic dysplasias is occupied by polycystic kidney disease. The occurrence of polycystic kidney disease is associated with a violation of the embryonic development of the kidneys, most often in the form of a lack of connection of the primary collecting tubules with a part of the nephron developing from a metanephrogenic blastoma. The blind tubules formed in this case continue to develop, primary urine accumulates in them, which stretches them, causing epithelial atrophy. At the same time, the connective tissue surrounding the tubules grows.
The size of cysts varies widely: along with small ones, visible only with a magnifying glass or even a microscope, there are large ones, up to several centimeters in diameter. A large number of thin-walled cysts in the cortex and medulla of the kidneys give them the appearance of a honeycomb when cut. Histologically, cysts are represented by dilated tubules with cubic epithelium or have the appearance of cavities with a thick connective tissue wall and sharply flattened epithelium. E. Potter (1971) described cysts associated with the expansion of the cavity of the Bowman's capsule of the glomeruli, without changing the tubules. Cysts can be empty or contain serous, protein fluid, sometimes stained with blood pigments, uric acid crystals. The stroma of the kidneys in polycystic disease is sclerotic, often with focal lymphoid cell infiltration, and in children under 1 year old - with foci of extramedullary hematopoiesis. Sometimes islands of cartilage or smooth muscle fibers are found in the stroma. The number and type of glomeruli and tubules located between the cysts may vary.
Symptoms renal dysplasia
Simple total dysplasia is often described in the literature as hypoplastic dysplasia. Among all congenital malformations of the urinary system, it accounts for 2.7%.
A distinction is made between aplastic and hypoplastic variants. In the case of aplastic renal dysplasia, in the case of bilateral lesions, death occurs in the first hours or days of life.
The hypoplastic variant is characterized by the early manifestation of urinary syndrome, characterized by mosaicism, and the early development of chronic renal failure.
Simple focal dysplasia is usually diagnosed by nephrobiopsy or autopsy. There are no clinical manifestations of the disease.
In simple segmental dysplasia, the dominant symptom is the development of persistent arterial hypertension already at an early age, which is more common in girls. Children complain of headaches, there may be convulsions, and changes in the vessels of the fundus develop early.
One of the main clinical symptoms is pain syndrome in the form of abdominal pain, polyuria and polydipsia appear quite early as manifestations of tubulointerstitial syndrome. In some cases, there is a lag in body weight and growth of children. Urinary syndrome is manifested by predominant proteinuria against the background of microhematuria and moderate leukocyturia.
Clinical signs of polycystic kidney disease appear in adolescence: lower back pain, palpation of a tumor-like formation in the abdominal cavity, arterial hypertension. Urinary syndrome is manifested by hematuria. Pyelonephritis often joins. Functionally, the kidneys are preserved for many years, then hyposthenuria, decreased glomerular filtration and azotemia appear.
Multilocular cyst (focal cystic dysplasia of the kidney) is a focal form of cystic dysplasia of the kidney and is characterized by the presence of a multi-chamber cyst in one of its poles, limited by a capsule from normal kidney tissue and divided internally by septa.
The clinical picture of a multilocular cyst is characterized by the appearance of pain syndrome of varying severity in the abdomen and in the lumbar region due to the disruption of urine outflow due to compression of the renal pelvis or ureter by a large cyst. In addition, due to possible compression of the abdominal organs, symptoms simulating their disease occur.
Clinical manifestations of medullary dysplasia usually develop after reaching the age of 3 years, more often at the age of 5-6 years the "Fanconi symptom complex" appears - polyuria, polydipsia, increased body temperature, delayed physical development, repeated vomiting, dehydration, acidosis, anemia, rapid progression of uremia.
The clinical picture of aplastic cystic dysplasia is determined by the condition of the second kidney, in which pyelonephritis often develops due to the presence of dysplasia in it.
Multicystic dysplasia may manifest itself with the presence of dull or paroxysmal pain in the abdomen, as well as in the lumbar region. Arterial hypertension may be detected.
In cortical dysplasia (microcystic kidney disease, congenital nephrotic syndrome of the "Finnish" type), the kidneys are not changed in size, lobulation may be preserved. Small glomerular and tubular cysts with a diameter of 2-3 mm are detected. The picture of nephrotic syndrome is observed from birth. Congenital nephrotic syndrome of the "Finnish" type is hormone-resistant, with an unfavorable prognosis. Early development of chronic renal failure is noted.
The clinical picture of hypoplastic cystic dysplasia is caused by pyelonephritis, the development of chronic renal failure, the rate of progression of which depends not only on the amount of preserved parenchyma of the hypoplastic kidney, but also on the degree of damage to the second non-hypoplastic kidney, but, as a rule, having dysplastic elements.
Hypoplastic dysplasia can be detected against the background of an intercurrent disease, while extrarenal syndromes may be absent or weakly expressed. Urinary syndrome is manifested by hematuria with moderate proteinuria. Manifestations of this disease are very heterogeneous. Often there can be a proteinuric variant with significant loss of protein, but edematous syndrome is relatively rare, even with significant proteinuria, and nephrotic syndrome is characterized as incomplete. Dynamic observation of the child shows that the clinical picture is subsequently characterized by nephrotic syndrome, the presence of tubulo-interstitial changes, often with the layering of urinary tract infection.
Children with hypoplastic dysplasia typically develop hypoimmune or immunodeficiency states, which explains the addition of severe and frequent intercurrent diseases with the progression of the pathological process in the kidneys. An important feature of this nephropathy is the absence of high blood pressure, hypotension is more common. An increase in blood pressure occurs already with the development of chronic renal failure.
The course of hypoplastic dysplasia is torpid, there is no cyclicity or wave-like nature of manifestations, drug therapy is usually ineffective.
Forms
Currently, there is no generally accepted classification of renal dysplasia. Most authors, based on morphological manifestations, distinguish between simple and cystic dysplasias, and by localization - cortical, medullary, corticomedullary. Depending on prevalence, focal, segmental, and total dysplasias are distinguished.
Depending on prevalence, there are total, focal and segmental forms of cystic dysplasia.
Among the total forms of cystic dysplasia, aplastic, hypoplastic, hyperplastic and multicystic variants are distinguished.
Polycystic disease manifests itself in two main forms, which differ in the nature of inheritance, clinical manifestations, and morphological picture - "infantile" and "adult" types.
Polycystic disease of the "infantile" type (small cystic kidney) has an autosomal recessive type of inheritance. The kidneys are significantly enlarged in size and weight. Numerous cylindrical and spindle-shaped cysts are determined in the cortex and medulla. The cysts are delimited by scant layers of connective tissue. Cysts are also found in the liver and other organs. Clinical manifestations depend on the number of affected tubules. With damage to 60% of the tubules, death from progressive uremia occurs in the first 6 months. The results of O. V. Chumakova (1999) do not confirm the classical concepts of early mortality in children with autosomal recessive polycystic disease and show that their life expectancy can be quite long, even with early detection of clinical symptoms. However, chronic renal failure develops earlier in them than in the autosomal dominant form of polycystic disease. In these patients, the leading role in the clinical picture is played by symptoms of liver damage. Micro-, macrohematuria and increased blood pressure are often observed in the clinic. Polycystic disease is often complicated by pyelonephritis with a torpid course.
In polycystic disease of the "adult" type (large cystic kidney), the kidneys are almost always enlarged in size, their mass in adults reaches up to 1.5 kg or more each. In the cortex and medulla there are numerous cysts up to 4-5 cm in diameter.
Diagnostics renal dysplasia
Diagnosis of polycystic kidney disease is based on family history, ultrasound data, excretory urography, which show an increase in the contours of the kidneys, flattening of the renal pelvis with elongation, lengthening and compression of the calyces.
In the diagnosis of multilocular cysts, radiological examination methods, including nephrotomography and angiography, are of decisive importance.
Among the laboratory signs of medullary dysplasia, hypoproteinemia is characteristic, the urinary syndrome is usually manifested by slight proteinuria. Due to increased loss of salts, hyponatremia, hypokalemia and hypocalcemia develop. Acidosis develops due to significant bicarbonaturia, a violation of acido- and ammoniogenesis.
Diagnosis of aplastic cystic dysplasia is based on ultrasound data, excretory urography, reno- and scintigraphy. During cystoscopy, the ureteral orifice on the side of the rudimentary kidney is usually absent or stenotic.
For the diagnosis of hypoplastic dysplasia, the accidental detection of the disease, the presence of multiple stigmas of dysembryogenesis, and some delay in physical development are of great importance.
How to examine?
What tests are needed?
Differential diagnosis
Treatment renal dysplasia
Treatment of hypoplastic dysplasia is symptomatic.
If multicystic disease is detected, a nephrectomy is performed due to the risk of developing malignancy.
Treatment of medullary dysplasia is symptomatic. In the development of chronic renal failure, hemodialysis or peritoneal dialysis and kidney transplantation are indicated.
Forecast
The prognosis for hypoplastic dysplasia is serious, with early development of chronic renal failure and the need for replacement therapy - hemodialysis or peritoneal dialysis, kidney transplantation.
[ 28 ]
Использованная литература