Medical expert of the article

New publications
Capillaroscopy
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Capillaroscopy is a method of visual examination of capillaries in vivo. The full name of the method is wide-field capillaroscopy of the nail bed. The study is carried out at low magnification of the microscope (x12-40), the object of observation is the distal row of capillaries of the nail bed (eponychium). The use of low magnification significantly expands the field of view, which makes it possible to study not only individual capillaries, but also the capillary network of a given area as a whole. The choice of the nail bed for examination is determined by the characteristic location of the capillaries in this area.
 [
[ What is capillaroscopy performed for?
Differential diagnosis of primary and secondary Raynaud's syndrome, early diagnosis of systemic scleroderma.
Interpretation of results
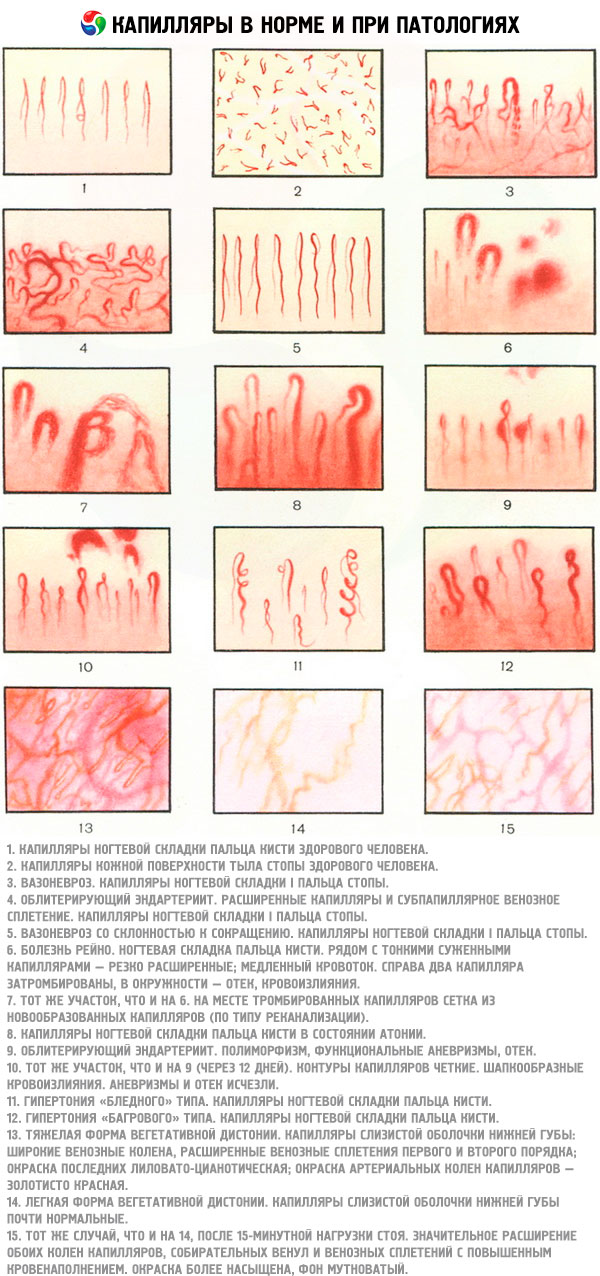
In healthy individuals, when performing capillaroscopy, the nail bed capillaries are a regular row of parallel, identical in size and shape, U-shaped loops, evenly distributed along the edge of the nail bed. Normally, there are 8 or more capillaries per 1 mm of the edge of the nail bed.
The main capillaroscopic signs of damage to microcirculatory vessels are changes in the size and number of capillaries. Most often, changes in size are manifested in the form of dilation of varying degrees of severity. The diameter most accurately reflects changes in size. The length of capillaries, due to individual characteristics, can vary significantly in individual people and therefore is not used as an evaluation criterion. As a result of destruction, a reduction in the capillary network is observed, that is, a decrease in the number over a certain area. A decrease in the number can be expressed to varying degrees, up to the formation of capillary-deprived, so-called avascular areas.
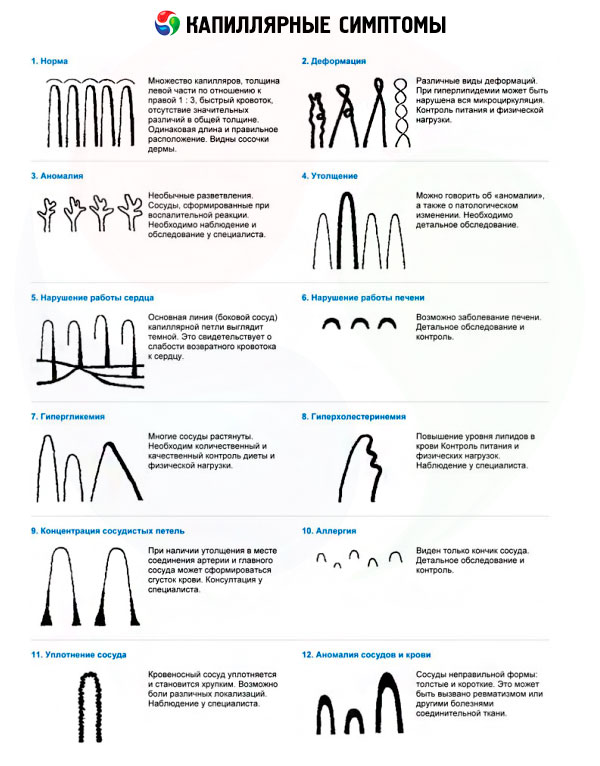
As a result of damage and disruption of the integrity of the capillary wall, erythrocytes are released into the perivascular space, where hemosiderin deposits are formed, which are visible during capillaroscopy as a series of sequentially located points between the top of the capillaries and the edge of the nail plate.
Less frequently, extravasates are represented by large confluent foci consisting of several small hemorrhages. Another important sign of damage to microcirculatory vessels is a change in the shape of the capillary loop. Pathologically altered capillaries can take on a bush-shaped, spiral or other shape. Bush-shaped capillaries are of the greatest importance. These are several capillary loops connected at the base and appearing as a consequence of new capillary formation. Their number reflects the intensity of neoangiogenesis.
Individual capillaroscopic signs and their combinations are characteristic of various diseases. Among systemic diseases of connective tissue, the greatest sensitivity and specificity of capillaroscopic changes are observed in systemic scleroderma. Signs characteristic of systemic scleroderma are varying degrees of dilation and decrease in the number of capillaries with the formation of avascular fields. In most cases, it is possible to identify dominant changes. Structural changes in capillaries in SSD reflect a certain stage of microangiopathy development.
Changes in capillaries and the capillary network progress in the following sequence: capillary dilation → capillary destruction → formation of avascular areas → growth of bushy capillaries → remodeling of the capillary network. Based on characteristic combinations of signs during capillaroscopy, capillaroscopic types of microangiopathy in SSD are distinguished:
- early type - a large number of dilated capillaries with a slight decrease in their number; avascular areas are either absent or isolated and of minimal degree;
- transitional type: reduced number of capillaries and simultaneous detection of dilated capillaries and avascular areas;
- late type - significant reduction of vessels and large avascular areas with single capillaries or complete absence of dilated capillaries.
For each type of microangiopathy, characteristic signs of activity are distinguished. Extravasates associated with dilated capillaries reflect the intensity of capillary destruction and microangiopathy activity in the early type of changes. In the late type, signs of microangiopathy activity (bushy capillaries) indicate intensive neoangiogenesis processes and are associated with avascular areas. In the transitional type, signs of microangiopathy activity are noted, characteristic of both the early and late types. Capillaroscopic changes are detected in the early stages of SSD and precede the development of characteristic clinical signs that determine the value of the research method in diagnosing the disease.
The great importance of capillaroscopy is in its ability to differentiate primary and secondary Raynaud's phenomenon, the first clinical manifestation of SSD. Unlike the Raynaud's phenomenon associated with SSD, in primary Raynaud's phenomenon capillaroscopic changes are absent or are represented by slight dilation of individual capillaries with their normal number. The severity and evolution of capillaroscopic changes correlate with the course of the disease and visceral pathology.
Characteristic capillaroscopic changes allow differentiating SSD from other diseases of the scleroderma group (diffuse eosinophilic fasciitis, scleredema of adults Buschke, scleromyxedema, generalized morphea), in which these changes are not detected. Along with this, capillaroscopy is of great importance in the differential diagnosis of SSD with Raynaud's phenomenon associated with other systemic diseases of connective tissue: dermato(loly)myositis, systemic lupus erythematosus and rheumatoid arthritis, the clinical manifestations of which in the early stages may be insufficiently specific. The most pronounced changes in the form of a large number of significantly dilated and bushy capillaries, avascular areas and massive extravasates are observed in dermato(poly)myositis. These changes are very similar to the changes observed in SSD, but are expressed to a greater extent. In dermato(poly)myositis, faster dynamics of capillaroscopic changes are observed compared to SSD, associated with the evolution of the disease. SSD-like changes in capillaries are also found in CTD. In some patients with SLE, capillaroscopy reveals moderately dilated capillaries, spiral deformation of capillaries, and an increased pattern of subpapillary plexuses, but the specificity of these changes requires proof. In RA, capillaroscopic changes are presented in the form of thinning (decrease in diameter) and elongation of capillary loops; the number of capillaries usually does not change.
Factors Affecting the Result of Capillaroscopy
Capillaroscopy may be difficult in patients with severe flexion contractures of the fingers.