Medical expert of the article

New publications
Beckwith-Wiedemann syndrome.
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Beckwith-Wiedemann syndrome (BWS) is a congenital disorder characterized by excessively rapid growth in infancy, asymmetry of body development, increased risk of cancer and some birth defects, and behavioral problems in children. It was first described as a familial form of omphalocele with macroglossia in 1964 by German doctor Hans-Rudolf Wiedemann. In 1969, J. Bruce Beckwith of Loma Linda University, California, described similar symptoms in several patients. Professor Wiedemann initially coined the term EMG syndrome to describe the combination of congenital umbilical hernia, macroglossia, and gigantism. Over time, this pathology was renamed Beckwith-Wiedemann syndrome (BWS).
Causes Beckwith-Wiedemann syndrome.
Beckwith-Wiedemann syndrome has a complex inheritance pattern, the disease locus is located on the short arm of chromosome 11 (CDKN1C, H19, IGF2, and KCNQ1OT1 genes). Abnormal methylation disrupts the regulation of these genes, which leads to excessively rapid growth and other characteristic features of Beckwith-Wiedemann syndrome.
About 1% of all people with this syndrome have chromosomal abnormalities, such as rearrangements (translocations), abnormal copying (duplication), or loss (deletion) of genetic material from chromosome 11.
Molecular genetic verification of changes in this locus is possible.
Symptoms Beckwith-Wiedemann syndrome.
The disease is characterized by premature rapid growth in the child at an early age. After 8 years of age, growth slows down. In some children with Beckwith-Wiedemann syndrome, individual body parts on one side may grow to abnormally large sizes (called hemihyperplasia), which leads to an asymmetrical appearance.
Some infants with Beckwith-Wiedemann syndrome have an abnormally large tongue (macroglossia), which sometimes makes breathing and swallowing difficult, abnormally large abdominal organs (splanchnomegaly), skin folds or pits near the ears, hypoglycemia, and kidney abnormalities.
Children have an increased risk of developing several types of cancer, particularly kidney cancer, Wilms tumor, and hepatoblastoma.
Complications and consequences
Possible complications in patients with Beckwith-Wiedemann syndrome:
- the probability of neonatal hypoglycemia (60%) with the development of seizures caused by transient hyperinsulinism;
- The high frequency (10-40%) of embryonic tumors, especially with nephromegaly or somatic asymmetry of the body, requires observation and ultrasound examination of the kidneys 3 times a year until the age of 3 years and subsequently 2 times a year until the age of 14 years (timely diagnosis of Wilms tumor).
 [ 15 ]
[ 15 ]
Diagnostics Beckwith-Wiedemann syndrome.
The diagnosis of Beckwith-Wiedemann syndrome should be considered in children with anomalies of the anterior abdominal wall (embryonic or umbilical hernia, divergence of the rectus muscles), macroglossia, neonatal hypoglycemia, and tumors (neuroblastoma, Wilms tumor, liver carcinoma).
Diagnostic criteria:
- Large birth weight or postnatal advanced physical development.
- Defects in the closure of the anterior abdominal wall (embryonic, umbilical hernia, diastasis of the rectus abdominis muscles).
- Visceromegaly (nephromegaly, hepatomegaly, splenomegaly).
- Macroglossia.
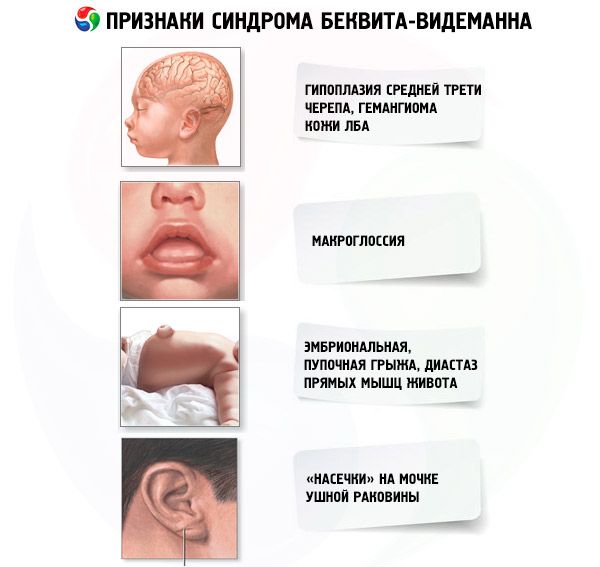
- Unusual face (hypoplasia of the middle third, hemangioma of the forehead skin, “notches” on the earlobe).
What tests are needed?
Treatment Beckwith-Wiedemann syndrome.
Defects of the abdominal wall are eliminated with the help of surgical treatment.
Hypoglycemia in neonates with BWS should be treated according to standard protocols for neonatal hypoglycemia management.
Macroglossia often becomes less noticeable with age and does not require any treatment. In severe cases, macroglossia can be corrected with surgery. Some surgeons recommend performing the surgery between 3 and 6 months.
In severe cases, hemihypertrophy is corrected using orthopedic methods.
[ 19 ]
Forecast
Beckwith-Wiedemann syndrome has a variable prognosis for life. It is determined by timely diagnosis of hypoglycemia (prevention of mental retardation) and early diagnosis of embryonic tumors.
Life expectancy is generally no different from that of healthy people.
Использованная литература