Medical expert of the article

New publications
Appendicular abscess: clinic, autopsy
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Acute appendicitis is a very common surgical pathology. This disease requires urgent surgical intervention, otherwise serious and life-threatening complications may develop. One of these complications is an appendicular abscess - suppuration in the area of the inflamed appendix.
 [ 1 ], [ 2 ], [ 3 ], [ 4 ], [ 5 ], [ 6 ], [ 7 ], [ 8 ], [ 9 ]
[ 1 ], [ 2 ], [ 3 ], [ 4 ], [ 5 ], [ 6 ], [ 7 ], [ 8 ], [ 9 ]
Epidemiology
Appendicular abscess is diagnosed relatively rarely: in approximately 0.1-2% of patients with acute appendicitis.
As a rule, an appendicular abscess develops in the first three days from the onset of the acute inflammatory process in the appendix, or occurs as a complication of the infiltrate (several days or weeks after its formation).
Causes appendicular abscess.
The development of an appendicular abscess occurs only when there is no correct or timely treatment of acute appendicitis. Unfortunately, it is impossible to predict acute inflammation in the appendix in advance. In addition, the pathology is often mistaken for other types of inflammatory processes in the abdominal cavity. Delaying time and incorrect diagnosis lead to the destruction of the inflamed tissues of the appendix, with the development of peritonitis or appendicular abscess. There are certain risk factors, the presence of which increases the risk of untimely detection of appendicitis, and, as a consequence, the formation of an appendicular abscess:
- Atypical localization of the appendix can lead to an initially incorrect diagnosis - inflammation of the kidneys, uterus, ovaries, enterocolitis, cholecystitis. As a result, the patient is offered treatment for other diseases instead of urgent surgical intervention. In this case, the diagnosis of appendicitis becomes clear only when an abscess forms.
- Strong antibacterial treatment at the time of initial inflammation in the appendix can lead to a decrease in the inflammatory reaction and the formation of a so-called “cold” abscess – a sluggish process that can take place over several years without disturbing the patient.
- Delayed seeking of medical care for acute appendicitis often leads to the development of an appendiceal abscess.
Pathogenesis
A distinction is made between a primary abscess, which occurs directly near the appendix, and a secondary abscess, which develops at some distance. The formation of an abscess is preceded by the appearance of an appendicular infiltrate - a kind of fence of the inflamed appendix from the abdominal cavity.
The formation of an infiltrate is a consequence of fibrin effusion and adhesions between the affected omentum, intestine, abdominal wall and appendix.
After the inflammation in the appendix subsides, the infiltrate is resorbed. But when the purulent process spreads beyond the vermiform appendix, the infiltrate becomes suppurated.
The location of the appendicular abscess depends on the location of the appendix. It is more favorable for the patient if the abscess forms in the iliac zone against the background of the lateral location of the appendix: it is in this position that the maximum separation of the inflamed area from the abdominal cavity is observed.
A secondary appendicular abscess forms somewhat differently. The purulent process, spreading to healthy tissues, affects the area of the mesentery of the small intestine, the area near the liver, diaphragm and right kidney. Secondary appendicular abscesses form in a similar way after resection of the appendix in destructive inflammation.
Symptoms appendicular abscess.
The onset of the development of an appendicular abscess differs little in its clinical course from acute appendicitis.
The first signs may look like this:
- the patient feels nauseous and may vomit;
- severe weakness appears;
- the pain in the abdomen is throbbing, it increases and becomes unbearable;
- bloating and increased gas formation are observed;
- body temperature rises.
When palpating the abdomen, the patient feels severe pain, but there are no symptoms of peritonitis. The body temperature is high (up to 40°C), accompanied by chills.
The listed symptoms may persist for 2-3 days.
Appendicular abscess in children
During the course of an appendicular abscess in children, doctors distinguish several stages, similar to peritonitis:
- Reactive stage – lasts about a day from the onset of inflammation. The stage is characterized by the appearance of general signs of an inflammatory reaction in the child. This may be a change in mood, vomiting, increased heart rate, febrile temperature. The pain in the abdomen increases, the abdominal muscles are tense when palpated.
- Toxic stage – lasts 1-3 days. Symptoms of severe intoxication and dehydration are evident: the child’s skin is pale, the eyes are shiny, and vomiting attacks become constant.
- The terminal stage is detected on the 3rd day and is characterized by damage to the entire body. First of all, internal organs suffer, signs of respiratory and cardiovascular failure occur.
After the reactive stage, the child's condition may erroneously improve - the pain will become less pronounced. However, after a while, the baby's health will sharply worsen. At the same time, there is a tendency: the older the child, the longer the period of false improvement can be.
Where does it hurt?
Complications and consequences
When an appendicular abscess develops, the speed of medical care is of great importance - the severity of the consequences depends primarily on this fact.
If medical assistance is not provided at all, or is provided too late, the patient may die.
Timely and qualified medical intervention provides every chance for the patient's full recovery.
The most likely complications of an appendiceal abscess may include:
- sepsis is a systemic inflammatory reaction;
- gangrenous lesion of internal organs;
- adhesive process;
- peritonitis;
- liver failure.
Most complications of appendicular abscess pose a serious danger not only to the health but also to the life of the patient. The reason for this is a purulent infection that spreads throughout the body in a short time.
Diagnostics appendicular abscess.
At the first signs of appendicitis, the patient must be immediately taken to a medical facility. The doctor will examine the patient, palpate the abdominal area and assess the patient's condition as a whole.
Diagnostic measures for suspected appendiceal abscess always include blood and urine tests.
A blood test will indicate the presence of a pronounced inflammatory process: increasing leukocytosis with a shift in the leukocyte formula to the left, and an accelerated ESR are detected.
Instrumental diagnostics may include ultrasound examination of the abdominal cavity, X-ray examination, and in complex cases – diagnostic puncture, laparocentesis (puncture of the peritoneum with removal of fluid) and laparoscopy.
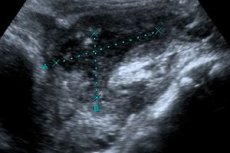
A sonographic sign of an appendicular abscess is the presence of an anechoic formation with irregular outlines, with detritus detected in its lumen. If the abscess is small, it is difficult to distinguish it from intestinal loops. To clarify the diagnosis, an ultrasound examination is performed in dynamics to determine the exact configuration of the intestine.
Differential diagnosis
Differential diagnosis of appendicular abscess is complex and is carried out with the following diseases:
- with food poisoning (especially with staphylococcal infection);
- with pre-perforated state of gastric ulcer and duodenal ulcer;
- with perforation of gastric ulcer;
- with an acute attack of cholecystitis;
- with hepatic colic in cholelithiasis;
- with acute inflammation of the pancreas;
- with acute enterocolitis;
- with acute ileitis (non-specific inflammation of the intestine);
- with diverticulitis and its perforation;
- with acute intestinal obstruction;
- with an acute inflammatory process in the uterus and/or appendages, with intrauterine pregnancy;
- with pelvic peritonitis;
- with right-sided renal colic or right-sided pyelonephritis.
Treatment appendicular abscess.
There should be no delay in treating an appendicular abscess, otherwise the abscess may burst, which will inevitably lead to the development of peritonitis. It is strictly forbidden to drink laxatives, anti-inflammatory and painkillers, as well as apply a warm heating pad to the abdomen with an appendicular abscess. At the pre-hospital stage, the patient should be provided with rest with mandatory bed rest. Cold can be applied to the abdomen.
The only correct and adequate treatment for an appendicular abscess is urgent surgical intervention, which consists of removing the abscess followed by drainage. During the operation, the surgeon removes dead tissue and cleans out the purulent cavity.
In the postoperative period, antibiotic therapy and wound rinsing with antiseptic solutions through installed drains are prescribed.
Medicines for appendiceal abscess
Ornidazole |
It is administered intravenously over 20 minutes, with an initial dose of 500-1000 mg every 12-24 hours. After the patient's condition has normalized, they switch to taking tablets in the amount of 500 mg every 12 hours. During the administration of the drug, dyspepsia, drowsiness, and headaches may occur. |
Cefepime |
Usually, Cefepime is administered 1-2 g intravenously every 12 hours, sometimes followed by metronidazole. If severe side effects such as skin rash, dyspepsia, and fever occur, the dosage of the drug may be changed. |
Ciprofloxacin |
Take 0.125-0.5 g orally twice a day for 5-15 days. Ciprofloxacin is usually well accepted by the body, but the possibility of allergic reactions should not be excluded. |
Ceftriaxone |
Prescribed 1-2 g daily. The duration of treatment is determined individually. Sometimes during treatment with Ceftriaxone, stomach upset occurs, the blood picture changes. As a rule, such phenomena disappear after the drug is discontinued. |
Vitamins
After the operation, during the rehabilitation period, the doctor will definitely prescribe vitamins to speed up healing and restore intestinal flora. To support the body, specialists advise drinking dried fruit compotes, rosehip infusion, etc. Additionally, you can take B vitamins, ascorbic acid, vitamin A.
Taking vitamin and mineral complex preparations helps to quickly recover after surgery:
- Vitrum is a multivitamin complex product that is most suitable for improving the body's condition in the postoperative period, as well as during intensive treatment with antibiotics and other potent drugs. Vitrum is taken immediately after meals, 1 tablet daily for several months.
- Alphabet is a multivitamin and polymineral product that perfectly replenishes the increased need for minerals and vitamins during a critical period for the body. Three tablets of different colors are taken per day, keeping a time interval of 4 hours between doses. Alphabet is taken during meals, for at least one month.
- Supradin is a drug recommended by doctors during illnesses and rehabilitation. Supradin is perfectly absorbed in the body, thanks to its effervescent form - it is enough to take 1 effervescent tablet daily, having previously dissolved it in 100 ml of water.
- Perfectil is a vitamin and mineral complex preparation that accelerates cell regeneration, normalizes cellular metabolism, and has wound-healing, antioxidant, and dermatoprotective properties. Perfectil is taken 1 capsule daily after meals, preferably in the first half of the day.
Physiotherapy treatment
After surgery for appendicular abscess, a number of effective physiotherapy methods are used, which helps speed up the rehabilitation of patients. At the same time, physical procedures that have a thermal effect are used extremely carefully.
First of all, physiotherapy procedures should be aimed at stimulating the healing process in the area of surgical intervention:
- infrared laser treatment;
- ultrasound treatment;
- peloid therapy;
- low frequency magnetic therapy;
- UHF treatment.
If the goal is to eliminate pain, then low-frequency electrotherapy, galvanization and medicinal electrophoresis are used.
Further treatment at a health resort, balneotherapy, and hydrotherapy are indicated.
Folk remedies
Folk recipes will come in handy during the postoperative recovery period. Time-tested remedies will help improve digestion, eliminate constipation and diarrhea, restore appetite, strengthen the immune system, and also stimulate rapid wound healing.
- Ginger root and fresh garlic cloves are effective products for eliminating the effects of inflammation and normalizing digestive processes. If you add grated ginger and garlic in small quantities to food 1-2 times a day, you can quickly recover from serious illnesses and operations.
- A mixture based on lemon juice and fresh honey will bring great benefits to the body. This mixture will improve digestion and strengthen the immune system. It is enough to drink 2-3 glasses of warm boiled water with the addition of 2 teaspoons of the medicinal mixture daily.
- If you drink burdock tea 3-4 times a day, you can prevent the development of the inflammatory process and improve your overall well-being after an illness. Burdock can be combined with dandelion, but only if the patient does not take medications that lower blood pressure.
It is recommended to include freshly squeezed juices in your daily diet, especially from beets, carrots, spinach or cucumber, and also drink a sufficient amount of warm, clean water - this will help prevent constipation, which is extremely undesirable during the rehabilitation period after an appendicular abscess.
[ 42 ], [ 43 ], [ 44 ], [ 45 ], [ 46 ], [ 47 ], [ 48 ]
Herbal treatment
In order to eliminate the effects of the inflammatory process and relieve pain, you can use treatment with medicinal plants. Infusions and decoctions based on herbs are a good and affordable remedy that will bring invaluable benefits to the body.
- Wormwood tincture can help at any stage of inflammation: in the morning before breakfast and at night, take 20 drops of tincture in 100 ml of water.
- Pour 1 tbsp of clover grass into 300 ml of boiling water and leave for 20 minutes. Drink 100 ml three times a day after meals.
- Prepare a medicinal mixture from equal parts of strawberry, raspberry and yarrow leaves. Brew 2 tbsp of the mixture in 1 liter of boiling water, leave for a quarter of an hour and drink throughout the day.
Teas based on mint, thyme, caraway, and chamomile also have a pain-relieving and calming effect. These teas are brewed instead of regular black or green tea and drunk little by little throughout the day. Such treatment can be continued for several weeks in a row.
Homeopathy
After surgery, homeopathic medicines can be added to the treatment:
- Lachesis – 6-hundredth dilution, 2 granules for 10 days;
- Bellis Perrenis - for severe postoperative pain, in low and medium dilutions, depending on the severity of the patient's condition;
- Hypericum – for severe postoperative pain and paresthesia, 6 or 30-hundredth dilution, depending on the severity of the patient’s condition;
- Gepar Sulphur – to limit purulent inflammation and improve the evacuation of pus, 3 or 6-hundredth dilution, depending on the individual characteristics of the patient.
Of course, homeopathy cannot and should not replace traditional medicine, but it effectively complements it, promoting rapid recovery of the body, without unnecessary stress and side effects.
Surgical treatment
The specifics of surgical treatment of appendicular abscess are determined depending on its location.
Most often, a skin incision of approximately 10 cm is made above the right inguinal ligament near the iliac crest and the superior anterior iliac bone. The skin, subcutaneous tissue, fascia, and external oblique abdominal muscle are dissected. The internal oblique and transverse muscles are separated along the fibers.
The volume and location of the abscess are examined using a finger. The appendix is removed only if it is completely accessible, since there is a risk of pus getting into the abdominal cavity.
The purulent cavity is cleaned and drained by inserting a tube wrapped in a gauze swab to prevent the formation of a pressure ulcer on the wall of the inflamed cecum. The tube is fixed to the skin, mainly in the lumbar region.
After surgery, treatment is aimed at preventing possible complications and activating the body's defenses.
Opening of appendicular abscess according to Pirogov
As a rule, an appendicular abscess is opened using the extraperitoneal approach according to Pirogov or Volkovich-Dyakonov.
Pirogov's dissection is used for an abscess located deep in the right iliac region. The surgeon dissects the anterior abdominal wall to the parietal peritoneum layer, from top to bottom and from right to left, approximately 10 mm medial to the superior horizontal iliac spine or 20 mm lateral to the Volkovich-Dyakonov incision. The parietal peritoneum is then separated from the inner region of the ilium, exposing the outer side of the abscess.
An autopsy according to Volkovich-Dyakonov is performed when the appendicular abscess is adjacent to the anterior abdominal wall.
After the abscess is opened and sanitized, if the appendix is found in it, it is removed. A tampon and drainage are installed in the purulent cavity. The abdominal wall is sutured to the drainage tube.
More information of the treatment
Prevention
To prevent the development of an appendiceal abscess, it is important to seek medical attention for any acute abdominal pain.
The inflammatory process is not always obvious, so it is necessary to pay attention to other suspicious symptoms: increased gas formation, increased temperature, nausea or diarrhea.
You can't leave your health to chance. Sometimes simple precautions can save a person's life. If you contact doctors in a timely manner, you can treat any disease at an early stage, preventing a number of possible adverse complications.
Forecast
During the inflammatory purulent process, spontaneous opening (rupture) of the appendicular abscess into the intestinal lumen, into the abdominal cavity or behind the peritoneum, less often into the cavity of the urinary bladder or vagina, and even less often outward may occur. Therefore, the course of the acute disease may become complicated, and such complications are extremely unfavorable for the health and life of the patient.
Based on this, the prognosis of such a pathology as appendicular abscess is considered very serious. Its consequences completely depend on how timely and competent the medical care was, how high-quality and timely the operation was.