Medical expert of the article

New publications
Uterine myoma in pregnancy: whether it is dangerous and its effect on the fetus
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.

Many women of childbearing age are diagnosed with a tumor developing in the muscular layer of the uterus – myoma. And a uterine myoma detected during an examination during pregnancy can have a significant impact on the process of bearing a child. Although for some women, asymptomatic myomas have virtually no impact on their daily life or pregnancy.
How problematic pregnancy will be in the presence of fibroids depends on the type, volume and location of this non-malignant formation.
Is pregnancy possible with fibroids?
When asked whether pregnancy is possible with fibroids, gynecologists answer in the affirmative, since uterine fibroids, as a rule, are not the main cause of reproductive dysfunction, that is, an obstacle to fertilization of the egg and implantation of the blastocyst into the endometrium of the uterus.
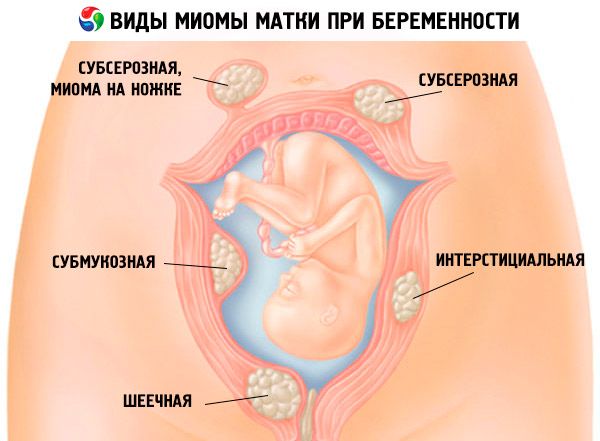
Although, everything depends on the location of the pathology development or the size of the formation (which varies from the size of a grain of wheat or a grape to a large apple). In most cases, a submucous or submucous myoma that enters the uterine cavity and disrupts its shape is incompatible with pregnancy. Such myomatous nodes are located in the muscles under the endometrium of the uterus, and having a myoma of this type, it is difficult to get pregnant.
Partially compatible are interstitial or, otherwise, intramural myoma arising inside the muscular layer of the uterus (between its layers) and pregnancy. A large myoma present in a woman can also be a cause of infertility: due to compression and blockage of the fallopian tubes, or localization at the transition of the cervix into its cavity.
But there are other types of myoma that have almost no effect on the intrauterine cavity. Thus, a subserous myoma facing the abdominal cavity and pregnancy are compatible. But this does not mean that there will be no problems during such a pregnancy: a subserous myoma can grow to a solid size, in addition, it can grow according to the papillary type, that is, it has a stalk (which can create its own problems, for example, its twisting).
Are uterine fibroids and ectopic pregnancy possible? The answer to this question is also affirmative: the development of an ectopic pregnancy due to the presence of fibroids is possible when the formation is localized in the area of the entrance of the fallopian tubes into the uterine cavity and blocks it.
It is also possible to plan a pregnancy with myoma. However, this does not mean preliminary removal of all nodes: a thorough examination should reveal nodes that will interfere with the normal course of pregnancy, and doctors recommend getting rid of such formations before pregnancy.
Causes uterine myomas in pregnancy
Although uterine fibroids are extremely common – with an overall incidence of up to 25% in women aged 30–35 years and twice as high in women aged 50 years – their exact etiology remains unclear.
Gynecologists associate the causes of the occurrence of these formations, including the causes of uterine fibroids during pregnancy as an intercurrent pathology, with excessive production of estrogen (17β-estradiol).
Risk factors
Risk factors for the development of fibroids: damage to the muscular layer of the uterine wall and its mucous membrane in inflammatory diseases of the reproductive organs, curettage of the uterine cavity (scraping during abortion), diagnostic manipulations on the uterus and appendages, as well as surgical interventions on the pelvic organs. In addition, experts include metabolic disorders (diabetes, obesity, hypothyroidism) among risk factors.
This pathology often has a familial nature (up to 20-25% of cases), which is explained by inherited point mutations of the ESR1 and ESR2 genes encoding estrogen receptors, and specific mutations of the MED12 gene (encoding the transcription factor of the protein synthesis enzyme).
 [ 5 ]
[ 5 ]
Pathogenesis
The pathogenesis is seen in the increased effect of estrogens on specific nuclear and membrane receptors of sex steroids in the tissues of the uterus (ERα and ERβ), the inadequate expression of which causes changes in the functions of the smooth muscle cells of the uterus (myocytes), stimulates their proliferation and, apparently, provokes a disruption in the synthesis of the main myofibrillar proteins (myosin and actin).
The structure of the multilayered muscular membrane of the uterus also contains a branched system of blood and lymphatic vessels, and the intercellular matrix contains connective tissue fibers of elastin and collagen. A violation of one of the structures, especially if there is multiple myoma or a large myoma during pregnancy, can lead to a decrease in the function of the myometrium, which ensures contraction and relaxation of the uterus, as well as its stretching during pregnancy.
It should also be borne in mind that during pregnancy, significant morphological changes occur in the structure of the myometrium, which are manifested in an increase in the number of myocytes (due to accelerated mitosis), an increase in their size (due to hypertrophy of cell nuclei) and increased collagen production.
Symptoms uterine myomas in pregnancy
At the initial stage of development of most types of this pathology, there are no symptoms. Myoma usually occurs before pregnancy, and the vast majority of women do not know about it: the formation is found during a gynecological examination or during an ultrasound examination.
With the onset of pregnancy, the growth of the formation may begin, and then such symptoms of uterine fibroids during pregnancy will appear as unpleasant feelings of discomfort, pressure, heaviness, or even pain if the formation presses on surrounding organs or pelvic structures. Sometimes such sensations are accompanied by a slight fever and nausea.
When the anterior wall of the uterus is affected by myoma, urination becomes more frequent, and when pregnancy and nodular myoma of the uterus on the posterior wall are combined, the problem of constant constipation arises.
Acute pain in the lower abdomen with myoma during pregnancy with irradiation to the lumbar region may be the result of nerve compression or a manifestation of the degeneration of the myoma into a cyst. The state of acute abdomen with fever and temporary leukocytosis occurs with a rare complication of myoma - internal hemorrhage in the tumor node (hemorrhagic infarction). And painful spasms in the abdomen or pain of a pulling nature are observed with twisting of the leg of a subserous myoma.
Pain is the most common symptom of fibroids later in gestation and occurs most often if a large fibroid forms during pregnancy (> 5 cm).
In the early stages, bleeding with myoma during pregnancy is associated with the localization of the formation: when the placenta is formed in close proximity to the node of hypertrophied tissue with submucous myoma. In fact, such bleeding is a miscarriage, that is, a spontaneous termination of pregnancy with uterine myoma.
Myoma also causes bloody discharge during pregnancy, when the myoma is large or grows in the thickness of the myometrium. Gynecologists say that myoma can cause a relapse of early miscarriage, which happens so early that the woman does not even know that she was pregnant.
Myoma growth during pregnancy
According to clinical observations using ultrasound, in almost a third of cases, fibroid growth is observed during pregnancy – especially during the first ten weeks. The average increase in tumor volume ranges from 6 to 18%, but in some pregnant women, fibroid growth is possible by 25-30% of the initial volume.
The growth of myoma during pregnancy depends on the individual characteristics of the woman's body and occurs under the stimulating effect of high levels of estrogen and other hormones produced by the placenta. Also, the increase in myoma nodes is largely due to the type and level of placental and pituitary growth factors (CYT) present in the blood.
Can myoma dissolve during pregnancy? Experts say that myoma never undergoes complete involution during pregnancy, but in almost 8% of cases it can decrease in the third trimester - up to 10%. But after childbirth, when the content of sex hormones in the blood decreases, the myomatous node can dissolve.
Complications and consequences
The main question is: how dangerous is myoma during pregnancy? Noting the negative impact of myoma on pregnancy, experts emphasize the special importance of preliminary (early) assessment of the degree of threat of complications. At the same time, they admit that it is almost impossible to predict how the tumor will behave and all that remains is to monitor how the pregnancy develops, regularly examining the pregnant woman's uterus using ultrasound.
The size of the fibroid and its location in the uterus are among the factors that determine the possibility of obstetric complications. Consequences and complications are especially often observed when fibroid nodes grow centripetally, that is, into the uterine cavity.
Spontaneous termination of pregnancy with uterine myoma occurs twice as often as in pregnant women without myoma. At the same time, as experience shows, multiple myoma during pregnancy - compared to the presence of a single nodular myoma - increases the frequency of miscarriages by three times. Early miscarriage occurs more often with submucous myoma, located in the upper part of the uterus, in which hypertonicity of the uterus develops.
Consequences and complications of myoma during pregnancy include placental abruption, particularly with retroplacental myoma (leading to ischemia of the decidual tissue of the placenta), submucous and multiple myomas; abnormal position of the fetus in the uterus and the need for cesarean section; premature onset of labor (especially common in the presence of multiple nodes or myoma that is adjacent to the placenta).
Necrosis of uterine myoma during pregnancy due to disruption of its tissue trophism may be an indication for emergency termination of pregnancy. For more details, see – Disruption of nutrition of uterine myoma node
Termination of pregnancy with myoma may also be necessary if it is impossible to reduce severe pain due to uterine distension; placental abnormalities and detachment; severe bleeding; very large myomatous nodes and uterine deformation, which are accompanied by spasm of the muscle fibers of the uterine wall.
Myoma and frozen pregnancy are associated with a disruption in the formation of the placenta, which causes prolonged oxygen starvation of the fetus and a cessation of its development.
Consequences of fibroids during pregnancy for the child
Another important question: what are the possible consequences of fibroids during pregnancy for the child?
In cases where uterine fibroids exert a compressive effect on the placenta, its functions are disrupted and placental insufficiency develops, which leads to fetal hypoxia (lack of oxygen) and hypotrophy (deficiency of nutrients). Due to which there is a delay in prenatal development.
Intrauterine growth retardation is associated not only with low birth weight of the child, but also with serious problems with independent breathing and thermoregulation, as well as the functioning of internal organs and the central nervous system.
In addition, under pressure from large fibroids, physical defects may occur in the form of twisting of the cervical spine, deformation of the shape of the skull, and anomalies of the bones of the limbs.
[ 19 ]
Diagnostics uterine myomas in pregnancy
Diagnosis of myoma during pregnancy may be associated with certain difficulties and give ambiguous results. Even experienced gynecologists detect only slightly more than 35% of large myomas (more than 5 cm) and 12-13% of small myomas (3-4 cm in size) during a routine examination.
Instrumental diagnostics using transabdominal ultrasound, according to the International Societies of Obstetrics & Gynecology, reveals myomas during pregnancy in 1.4-2.7% of cases, primarily due to the difficulty of differentiating myoma from physiological thickening associated with the menstrual cycle, local contraction of smooth muscle fibers of the myometrium, as well as from diffuse adenomyosis of the uterus. MRI is more informative, but pregnant women can undergo it only in the second and third trimesters. This diagnostic method is used only in complex cases.
What do need to examine?
How to examine?
Differential diagnosis
Differential diagnostics of myoma in pregnant women is intended to prevent cases when "through oversight" myoma is confused with pregnancy during palpation examination of the uterus. It is also necessary to differentiate myoma during pregnancy from other formations in the uterus, such as endometrial cysts or polyps.
Who to contact?
Treatment uterine myomas in pregnancy
The main treatment for uterine fibroids during pregnancy is symptomatic therapy and constant monitoring of the pregnant woman’s condition and the behavior of the fibroid.
In gynecological practice, hormonal drugs containing progesterone analogues - Duphaston and Utrozhestan - are prescribed for endometriosis (to neutralize the effect of estrogen on the receptors of the uterine mucosa), as well as in cases of threatened miscarriage (to achieve hormonal balance). They are not used to treat fibroids: Utrozhestan and Duphaston for fibroids during pregnancy (and in the absence thereof) are capable of causing accelerated proliferation of myometrial cells. Also read - Duphaston during pregnancy
From the second trimester, if there is no constipation or increased gas formation, iron-containing drugs can be prescribed: Gino-tardiferon (one tablet per day), Maltofer (100-200 mg once a day), etc. Pregnant women with fibroids also need vitamins B6, B9, B12.
To improve blood supply to the placenta and prevent its dystrophy, Curantil (Dipyridamole) is used - for more details, see Curantil during pregnancy
As a rule, surgical treatment – removal of myoma during pregnancy (myomectomy) – is not performed during pregnancy due to the high risk of damage to the uterus and miscarriage. Enucleation of the node in case of subserous myoma can be performed only in case of its necrosis.
Laparoscopy of uterine fibroids and pregnancy. The operation requires general anesthesia and three to four abdominal wall punctures; it is difficult to avoid termination of pregnancy, so such intervention is performed only in emergency cases.
Forecast
The prognosis regarding the course of pregnancy and its outcome with a small myoma is quite favorable (although doctors cannot guarantee the absence of complications). A consolation for pregnant women is that after the birth of the child, the enlarged uterine myoma during pregnancy almost always decreases in size, which gives them the opportunity to become a mother again.