Medical expert of the article

New publications
Intestinal obstruction in an infant: signs, treatment
Last reviewed: 04.07.2025

All iLive content is medically reviewed or fact checked to ensure as much factual accuracy as possible.
We have strict sourcing guidelines and only link to reputable media sites, academic research institutions and, whenever possible, medically peer reviewed studies. Note that the numbers in parentheses ([1], [2], etc.) are clickable links to these studies.
If you feel that any of our content is inaccurate, out-of-date, or otherwise questionable, please select it and press Ctrl + Enter.
Intestinal obstruction in newborns is an acute surgical pathology, which, if not treated in a timely manner, has many complications. There are different types of this disease, but their symptoms are similar, which allows you to suspect the problem in advance even at the initial stage. Therefore, parents should know about the symptoms and manifestations of the pathology in order to seek help in time.
 [
[ Epidemiology
Statistics of prevalence show that intestinal obstruction is a common disease - about 10% of acute abdominal diseases are caused by this pathology. In 0.1 - 1.6% it complicates the course of the postoperative period in sick children who have undergone operations on the abdominal organs in the neonatal period. The pathology is somewhat more common in boys. Mortality in this pathology ranges from 5 to 30% and strongly depends on gestation and age of the newborn. In the case of acute intestinal obstruction in the early postoperative period it reaches 16.2 - 60.3%, and depends on timely diagnosis, timing of surgical treatment.
Causes intestinal obstruction in newborns
Intestinal obstruction is a syndrome that complicates the course of many diseases and conditions. The pathophysiological link is the disruption of the movement of chyme along the digestive tract, which in turn completely or partially disrupts the motor function of the intestine. There can be many reasons for this, but it is the disruption of normal intestinal function that is one of the most important factors.
To understand all the reasons for the development of obstruction, it is necessary to know some types of this pathology. There are strangulation, obstructive, spastic and paralytic obstruction. Accordingly, different reasons are distinguished.
Obstructive obstruction occurs as a result of coprostasis or intestinal tumors, which is much less common in newborns. The cause of coprostasis is congenital Hirschsprung's disease, stenosis of the colon, which is accompanied by intestinal atony. This complicates the contraction and motility of the intestine from the very birth of the baby. This leads to the fact that such children suffer from constipation, and coprolites (small fecal stones) are formed from feces. Such coprolites can completely obstruct the lumen of the intestinal tube and cause intestinal obstruction.
Strangulation intestinal obstruction develops against the background of Meckel's diverticulum, internal hernias, especially clinically significant diaphragmatic hernias. Such pathologies often lead to increased intestinal motility, and especially in newborns, the intestinal mesentery is very mobile. This easily leads to compression of the intestinal wall and a kind of external strangulation occurs.
The most common causes of intestinal obstruction in newborns are diseases of other organs. They underlie the so-called paralytic obstruction. The reasons for it may be the following:
- medications, especially narcotics, that affect the muscular wall of the intestine;
- abdominal infection weakens not only motility, but also other functions of the intestine;
- mesenteric ischemia against the background of congenital pathologies of the vessels of the descending aorta or mesenteric arteries;
- complications of abdominal surgeries;
- diseases of the kidneys and chest organs;
- metabolic disorders (hypokalemia);
- necrotic enterocolitis in newborns;
Often such obstruction occurs against the background of birth trauma, functional immaturity of the digestive tract, pneumonia, sepsis, peritonitis. These pathologies cause a reaction of internal organs in the form of centralization of blood circulation, which causes ischemia of the intestinal wall. Peristalsis is also disrupted against the background of intoxication, especially in newborns against the background of immaturity of the mechanisms of coordination of this function. This leads to intestinal paresis and the further development of obstruction.
Intussusception is singled out separately, since this type of obstruction has elements of obstruction and strangulation. Intussusception is a special type of acquired obstruction in young children, the essence of which is that the proximal segment of the intestine is wedged into the distal one. Subsequently, the blood supply to the intestine is disrupted, which leads to its necrosis.
Intussusception may be caused by lymphadenopathy due to bacterial or parasitic disease. The mechanism of intussusception in infants is explained by the discoordination of peristalsis, which is caused by the uneven development of the longitudinal and circular muscles of the intestine.
A distinction is made between small-to-small intestinal intussusception, ileocecal type (90%), and very rare large-to-large intestinal (1-3%) intussusception. In the area where intussusception has occurred, a tumor-like formation is formed, which consists of three layers of the intestinal wall: the outer one, into which the intussusception is wedged, the middle one, and the inner one. Between these walls of the intussusception, the mesentery of the intestine is pinched. The clinical course of the disease depends on the degree of pinching - with mild pinching, symptoms of the obstruction process predominate, the disease proceeds easily, and intestinal necrosis does not occur. In cases of severe pinching, signs of strangulation intestinal obstruction predominate, bloody stools and necrosis of the intussusception quickly appear. Ileocecal intussusception proceeds more easily than small-to-small intestinal intussusception. After the phase of venous congestion, as a rule, the swelling rapidly increases, stagnant bleeding occurs, and bloody effusion appears in the abdominal cavity. Due to the progressive disruption of blood supply, necrosis of the intussusception occurs.
Risk factors
Taking into account all the causes of obstruction, we can identify risk factors for this pathology:
- low birth weight and associated intestinal immaturity;
- birth injuries;
- intestinal developmental abnormalities;
- severe infectious diseases of the intestines and other organs, sepsis.
Pathogenesis
The pathogenesis of changes in obstruction does not depend on its type, but depends on the local stoppage of food movement through the intestines. This causes further changes that underlie the development of symptoms.
In the area of the pathological source in the intestine, the integrity and permeability of the blood vessels and the peritoneum itself, which provide ultrafiltration of plasma and tissue fluid, are disrupted. This leads to the fact that plasma proteins containing inactive components of the blood coagulation system go beyond the vascular bed and peritoneum into the abdominal cavity. These substances are activated upon contact with the damaged peritoneum and tissues of the abdominal organs, a cascade coagulation reaction occurs, which ends with fibrin deposition on the surface of the abdominal organs. This is facilitated by tissue coagulation factors contained in the cells of the tissues of the abdominal organs and the peritoneal mesothelium. Fibrin deposited on the surface of the abdominal organs has adhesive properties and fixes adjacent organs. This leads to the fact that in the place where the food stopped, even more adhesion of the intestinal layers, as well as the mesentery, occurs. This completely disrupts the movement of chyme and is the main mechanism of the pathogenesis of intestinal obstruction in a newborn.
Symptoms intestinal obstruction in newborns
Symptoms of intestinal obstruction in newborns do not depend on the type, since the pathogenetic features of the course of the pathology do not have any special differences. The stages of development of disorders in intestinal obstruction go sequentially from impaired blood circulation in a certain section of the intestine to its necrosis. Considering that the intestinal wall in newborns is very thin, the period of development of symptoms is reduced. When intestinal necrosis occurs, the entire process ends in peritonitis.
The first signs of acute intestinal obstruction begin suddenly and are characterized by a large polymorphism of clinical manifestations. The process quickly leads to severe intoxication, changes in homeostasis, causes various complications of the pathological process and worsens the patient's condition.
The classic clinical picture of intestinal obstruction in a newborn is characterized by a sudden onset against the background of complete health. Pain in the intestines gradually develops, which is characterized by attacks of anxiety in newborns with the gradual addition of toxicosis.
Vomiting is one of the obligatory symptoms of this disease in newborns. With high intestinal obstruction, vomiting appears on the first day of life after birth. Depending on the level of damage, the nature of vomiting may vary.
Thus, in conditions of complete obstruction, the vomit will look like curdled milk without any bile. If the process is localized a little lower at the level of the distal parts of the small intestine, then the vomit will be digested milk.
The nature of the newborn's stool also changes. With high obstruction, almost normal meconium will pass, normal in quantity and color. If the obstruction process is slightly lower, then the meconium is practically not colored. There may also be bloody discharge from the rectum or streaks of blood in the child's stool.
The general condition of newborns from the onset of the disease is satisfactory, but quickly
Exicosis and hypotrophy phenomena progress against the background of repeated vomiting and diarrhea. Dryness of the skin, sunken eyes, fontanelle, decreased tissue turgor appear. Later, swelling of the epigastrium is noted, which decreases after vomiting.
The clinical picture of paralytic intestinal obstruction is characterized by severe abdominal distension, intoxication, stool retention and gas. Since the paralytic focus is wider than in other types of obstruction, the child's abdominal distension is very pronounced. This can disrupt the breathing process, which in turn can be a prerequisite for the development of hypoxia and hypostatic pneumonia.
Body temperature does not rise often; intoxication phenomena are often accompanied by dehydration and electrolyte disturbances.
Congenital intestinal obstruction in a newborn has the same symptoms, but they appear immediately after the birth of the child. Vomiting, impaired meconium passage, bloating - all these symptoms begin to appear within a few hours after birth.
Partial intestinal obstruction in a newborn is characterized by disorders in which the intestinal cavity is blocked only halfway. Therefore, the symptoms do not develop so acutely and must be carefully differentiated from functional disorders in newborns.
Complications and consequences
The consequences and complications of intestinal obstruction can be very serious. Considering intestinal necrosis in the absence of timely treatment, one of the most common consequences is peritonitis. More remote consequences can develop if surgical treatment was performed. In this case, dense adhesions are often formed, which can lead to repeated obstructions in the future. Persistent functional disorders of the intestine in children in the future are one of the common consequences of intestinal obstruction. If newborns with obstruction have other concomitant pathologies, the risk of mortality increases, including fatal complications.
Diagnostics intestinal obstruction in newborns
Diagnosis of intestinal obstruction in newborns must necessarily be based on a thorough examination of the baby. After all, vomiting and stool disorders are non-specific symptoms that are characteristic not only of intestinal obstruction.
It is imperative to examine the abdomen of a newborn baby if any intestinal pathology is suspected.
In case of intussusception, there are other local symptoms against the background of intestinal manifestations. A tumor-like formation of doughy consistency is palpated, which can change its position when pressed. In case of paralytic obstruction, the abdomen looks sharply swollen, soft when palpated. High tympanitis is detected during percussion, peristaltic noises are not heard during auscultation. The normal motility process is disrupted, therefore no noises are detected.
The tests that are necessary to diagnose obstruction are not specific, so at the initial stages they are limited to only general tests.
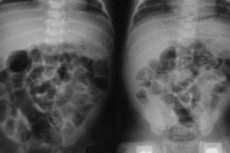
Instrumental diagnostics is the main and priority method for confirming the diagnosis of obstruction. X-ray examination allows us to determine the level of obstruction and its degree, because gases and food accumulate above the obstruction, and there are no signs of normal motility below. X-ray examination helps to verify changes characteristic of high intestinal obstruction: pronounced accumulation of air in the upper parts of the intestine and determination of the level of fluid under these gases. The intestinal loops are arranged in such a way that they form "arcades" that look like garlands filled half with air and half with liquid. A normal intestine has a clear distribution and location of loops.
What do need to examine?
How to examine?
Differential diagnosis
Differential diagnostics should be carried out with congenital intestinal anomalies, esophageal atresia, pyloric stenosis. All these pathologies are symptomatically very similar, but a thorough examination can determine the diagnosis.
Who to contact?
Treatment intestinal obstruction in newborns
If intestinal obstruction is suspected, hospital treatment of the child is mandatory. Therefore, if repeated vomiting or stool disturbances occur, it is necessary to hospitalize the newborn if he or she was previously at home. If the newborn begins to have such problems immediately after birth, it is necessary to consult a surgeon.
During the first 1.5-2 hours after the child is hospitalized, complex conservative therapy is performed. Such treatment has differential diagnostic value and by its nature can be preoperative preparation.
The therapy is aimed at preventing complications associated with pain shock, correcting homeostasis and, at the same time, is an attempt to eliminate intestinal obstruction using non-surgical methods.
- Measures aimed at combating abdominal pain shock include: neuroleptanalgesia (droperidol, fentanyl), paranephric novocaine blockade and administration of antispasmodics (baralgin, spazmoverin, spasfon, no-shpa). In children, the use of some drugs may be limited in the neonatal period, so treatment is carried out with mandatory consultation with a pediatric anesthesiologist. Pain relief is carried out after the diagnosis has been established.
- Elimination of hypovolemia with correction of electrolyte, carbohydrate and protein metabolism is achieved by introducing salt blood substitutes, 5-10% glucose solution, gelatin, albumin and blood plasma. All calculations are made taking into account the needs of the newborn baby's body for fluid, and in addition, the needs for nutrients are also taken into account.
- Correction of hemodynamic parameters, microcirculation and detoxification therapy are carried out using intravenous infusion of rheopolyglucin, rheogluman or neohemodesis.
- Decompression of the gastrointestinal tract is performed using a nasogastric tube. A child with a confirmed diagnosis of intestinal obstruction should be transferred to total parenteral nutrition. Feeding the child is prohibited and all substances are calculated based on body weight. At the time of treatment, enteral nutrition is completely prohibited; from the moment of recovery, breastfeeding is gradually introduced.
- In the treatment of paralytic obstruction, it is necessary to treat the underlying disease that caused the paresis. In addition, medicinal stimulation of intestinal peristalsis is carried out with proserin and infusion solutions.
When there is an obstruction, then gradual necrosis with absorption of decay products and intoxication necessarily occurs in this section of the intestine. This is always a prerequisite for the proliferation of bacteria, therefore, regardless of the method of treatment, antibacterial therapy is used for intestinal obstruction. Only spastic and paralytic obstruction is treated with conservative methods for several hours. All other types of obstruction must be treated by surgical intervention without delay. In this case, initial antibacterial, infusion therapy is carried out for two to three hours, which is preoperative preparation.
- Sulbactomax is a combination antibiotic that consists of the 3rd generation cephalosporin ceftriaxone and sulbactam. This composition results in the antibiotic becoming more stable and not being destroyed by bacteria. This drug is used for treatment in combination with other drugs. The method of administration is intravenous for faster action. The dosage of the drug is 100 milligrams per kilogram of body weight. Side effects include allergic reactions, renal dysfunction, and effects on the liver.
- Kanamycin is an antibiotic from the macrolide group, which is used for newborns in the treatment of intestinal obstruction both preoperatively and in the postoperative period to prevent complications. The dosage of the drug is 15 milligrams per kilogram of body weight per day for the first three days, then the dose can be reduced to 10 milligrams. Method of administration - intravenous or intramuscular, divided into 2 doses. Side effects can be in the form of irreversible hearing loss, as well as toxic effects on the kidneys.
When the child's condition stabilizes, mandatory surgical intervention is performed. Surgical treatment of intestinal obstruction is mandatory for obstructive and strangulation types. Since these types have a mechanical obstruction, it is impossible to restore normal intestinal function with medications alone.
After a short preoperative preparation of the child, anesthesia is administered. In such cases, general anesthesia is used for a newborn.
The main goal of surgical intervention is to eliminate the obstruction, restore normal bowel function, eliminate bowel necrosis and sanitize the abdominal cavity.
The surgical technique is as follows. The incision is made along the midline of the abdomen, along the balls, while stopping the bleeding. After the peritoneum is incised, the cavity is inspected and the obstruction is identified. As a rule, the lesion is immediately visible by the changed color of the intestine. The affected intestine is examined along its entire length and at a distance of several tens of centimeters from this lesion. If perforation has not yet occurred, the intestine may not be seriously damaged, in which case the obstruction is simply removed. This may be a volvulus, obstruction by fecal stones. If necrosis of a section of the intestine has occurred, then resection of this section is mandatory. The vital activity of such an affected section of the intestine can be determined by its color, reaction to irritation. After resection, sections of the healthy intestine are sutured. After this, the abdominal cavity is sanitized with antiseptic solutions, and if there was intestinal necrosis, drains are installed.
The early postoperative period is carried out with drug support with antibiotics and infusion solutions.
Intussusception is a special type of obstruction and its treatment is slightly different. If intussusception was diagnosed during the first 24 days after its onset, then conservative treatment is possible. For this purpose, air insufflation through the rectum under pressure is used. Such an air flow allows the intussusception to be straightened without surgical intervention.
Traditional methods of treating intestinal obstruction are not used in newborns.
Prevention
Prevention of obstruction consists of monitoring the risk group for the development of this pathology, as well as careful care of premature babies not only by the staff, but also by the parents. After all, parents are the first to notice any changes and symptoms in the child.
Forecast
The prognosis for survival is favorable in more than 80% of cases, provided that diagnosis is made in a timely manner without the development of complications.
Intestinal obstruction in newborns is a pathology of impaired food movement through the intestines, which is associated with a real obstacle, externally or internally located. Symptoms usually occur acutely immediately after the first intestinal damage. Therefore, it is important for parents to know the main manifestations of the pathology and, in case of danger, seek help in time.